Vaginal Odour: 7 Proven Causes That Aren’t Poor Hygiene (And When to See a Specialist)
The Moment That Sends You Spiralling
You notice it in the afternoon. Maybe after a workout, maybe while changing your clothes, maybe just quietly, in the middle of an ordinary day. There is a scent, unfamiliar, slightly off, and immediately your brain runs a terrible little checklist.
Did I shower this morning? Did I use the wrong soap? Is something wrong with me?
You scrub harder in the shower that night. You switch your underwear to something breathable. You buy a different wash, maybe something labelled “feminine freshness,” and for a few days it seems better. Then it comes back. And now you are not just uncomfortable. You are embarrassed. Possibly even ashamed.
Here is what I need you to hear before we go any further: vaginal odour that persists, changes, or causes you anxiety is almost never about hygiene. It is almost always a physiological signal. Your body is communicating something specific, something with a real clinical name and a real clinical explanation, and it deserves to be taken seriously instead of washed away.
You are not unclean. You are not broken. You are, almost certainly, dealing with something far more common and far more treatable than you have been led to believe.
Let us talk about what is actually happening.

What Vaginal Odour Actually Tells You: The Clinical Foundation
The vagina is a self-regulating ecosystem. It maintains its own pH (the measure of acidity versus alkalinity, on a scale from 0 to 14), its own microbial community, and its own defence mechanisms. A healthy vaginal environment is naturally slightly acidic, typically between pH 3.8 and 4.5, which is roughly the same acidity as a glass of wine or a cup of black coffee.
Think of it like a garden. When the soil pH is balanced, the right plants thrive and weeds struggle to take hold. When that balance shifts, even slightly, the entire ecosystem responds. The same is true for the vaginal microbiome.
The dominant bacteria in a healthy vagina belong to the Lactobacillus genus. These bacteria produce lactic acid, which keeps the pH low and actively suppresses the growth of harmful organisms. When Lactobacillus populations are disrupted, the pH rises, opportunistic bacteria multiply, and one of the most noticeable results is a change in scent.
Vaginal odour, therefore, is not a hygiene failure. It is frequently the first, most detectable signal of a microbial or hormonal shift inside the body, and it warrants investigation rather than concealment.
This topic is chronically underserved in mainstream medicine for a painfully simple reason: women are frequently told to manage the symptom rather than investigate the cause. Scented products are recommended. Douching, despite being clinically contraindicated, is still widely practised. The underlying physiology is too often left unexamined.
The key point: A persistent change in vaginal odour, particularly one accompanied by discharge, itching, or discomfort, is a clinical sign. It should prompt a conversation with your gynaecologist, not a trip to the feminine hygiene aisle.
7 Causes of Vaginal Odour That Have Nothing to Do With Hygiene
FORMAT B: Root Causes and Their Clinical Mechanisms
Understanding why your body is producing a particular scent is the first step toward addressing it properly. Each of the following causes has a distinct mechanism. Knowing the difference can save you months of misdiagnosis and misdirected self-treatment.
1. Bacterial Vaginosis: The Most Misunderstood Culprit
Bacterial vaginosis, commonly known as BV, is the single most common cause of unusual vaginal odour in women of reproductive age, yet it is also one of the most persistently misunderstood conditions in women’s health.
BV is not an infection in the traditional sense. It is a dysbiosis, meaning a disruption of the normal microbial balance inside the vagina. When protective Lactobacillus bacteria are displaced by a diverse overgrowth of anaerobic bacteria (organisms that thrive without oxygen), such as Gardnerella vaginalis, Prevotella, and Mobiluncus species, the vaginal pH rises above its healthy range. These anaerobic bacteria produce volatile compounds called amines, including trimethylamine and putrescine, which generate the characteristic fishy or musty odour associated with BV.
Critically, BV is not caused by poor hygiene. In fact, excessive cleaning, particularly with soap, scented washes, or by douching, actively disrupts the Lactobacillus colonies that would otherwise prevent BV from developing. Washing inside the vagina removes the protective acid layer the body has worked to maintain. It is counterproductive in the most literal sense.
Research consistently shows that BV affects between 20 and 30 percent of women of reproductive age at any given time, making it extraordinarily common. Yet many women remain undiagnosed for months or years because the odour is dismissed or because they do not present with the classic white-grey discharge that textbooks describe. Some women with BV experience no discharge at all. The odour alone, particularly after sex or during menstruation when pH naturally fluctuates, can be the only symptom.
According to Mayo Clinic’s guidance on bacterial vaginosis, BV can increase the risk of sexually transmitted infections and complications during pregnancy, making accurate diagnosis and appropriate treatment clinically important. It is not merely cosmetic.
Standard treatment involves either oral or topical antibiotics, most commonly metronidazole or clindamycin, and increasingly, attention to vaginal microbiome restoration is being incorporated into treatment plans.
If the odour you are experiencing is fishy, strongest after sex, and accompanied by a thin, greyish discharge, BV should be your first conversation with your gynaecologist.
2. Hormonal Fluctuations: When Oestrogen Drives the Shift
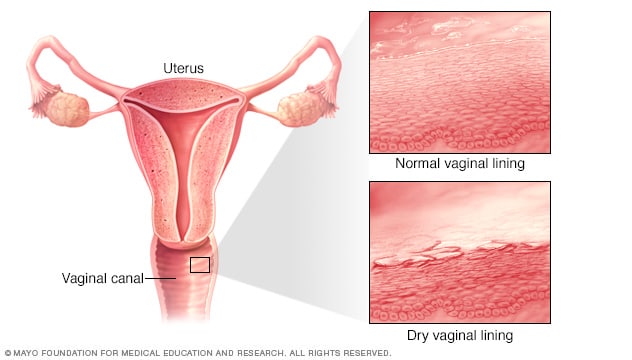
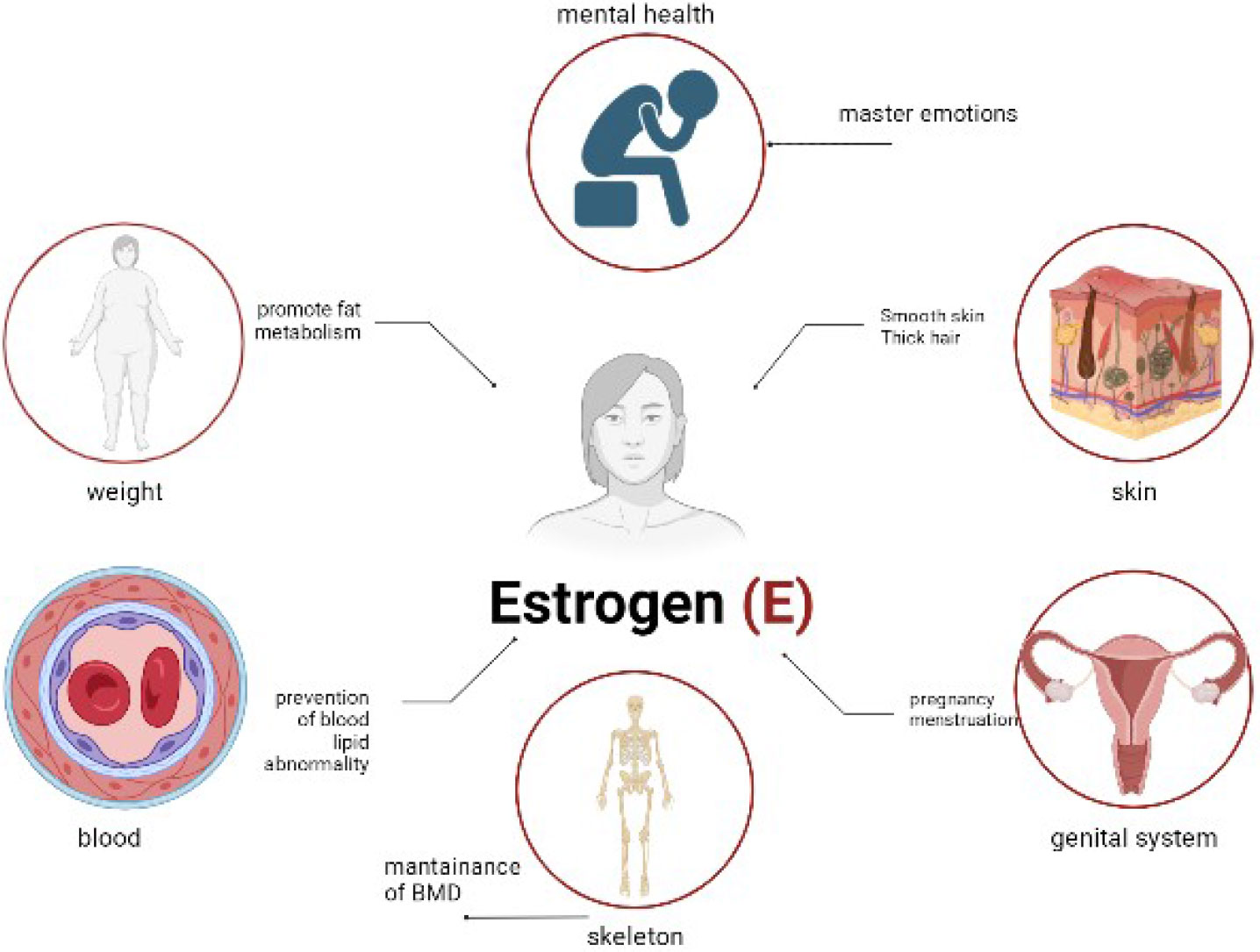
The vaginal microbiome does not exist in a vacuum. It is intimately regulated by oestrogen, the primary female sex hormone that orchestrates everything from the thickness of the vaginal lining to the survival of Lactobacillus bacteria.
Here is the mechanism: oestrogen stimulates vaginal epithelial cells (the cells lining the vaginal wall) to produce glycogen, a form of stored sugar. Lactobacillus bacteria feed on glycogen to produce lactic acid, which in turn maintains the vaginal pH within its protective acidic range. When oestrogen levels fall, as they do during certain phases of the menstrual cycle, during the postpartum period, during perimenopause, or during menopause itself, glycogen production decreases. Lactobacillus populations shrink. The pH rises. And the door opens for odour-producing bacteria to proliferate.
This is why many women notice a change in vaginal scent at predictable times: just before and during menstruation, when oestrogen is at its monthly low point. It is also why women in perimenopause or postpartum recovery frequently report vaginal odour that they have never experienced before, alongside dryness, irritation, and changes in discharge.
Breastfeeding suppresses oestrogen particularly dramatically. If you are a new mother and noticing a change in vaginal scent, this is almost certainly contributing. It is physiological, expected, and temporary, though it does deserve attention and support.
The clinical term for the vaginal changes associated with low oestrogen is genitourinary syndrome of menopause (GSM) in older women, and atrophic vaginitis in its more acute form. Both can produce odour changes without any infection being present.
If your odour changes are cyclical, if they worsen in the luteal phase of your cycle, during breastfeeding, or since entering perimenopause, the conversation to have is about hormonal support, not antibiotics.
3. Trichomoniasis: The STI That Frequently Goes Unnoticed
Trichomoniasis, often called “trich,” is a sexually transmitted infection caused by a single-celled parasite called Trichomonas vaginalis. It is one of the most common curable STIs in the world, yet it is also one of the most underdiagnosed, because a large proportion of people who carry it, estimates suggest up to 70 percent, experience no symptoms at all.
When symptoms do occur in women, they typically include a frothy, yellow-green vaginal discharge and a strong, unpleasant odour that is often described as musty or foul. The mechanism behind the odour is similar to BV: the parasite disrupts the vaginal ecosystem, elevates pH, and creates conditions that favour odour-producing anaerobic bacteria. Trich can also co-exist with BV, compounding both the odour and the discharge.
What makes trichomoniasis particularly relevant here is that it is frequently treated as BV when first assessed, because the odour and discharge can seem similar. If you have been treated for BV more than once without lasting resolution, and particularly if you are sexually active, it is worth requesting a specific test for Trichomonas vaginalis. Standard vaginal swabs tested for BV will not automatically detect trich. You need to ask for it.
Treatment is straightforward: a single dose of metronidazole or tinidazole is highly effective. Both partners need to be treated simultaneously to prevent reinfection, which is an important step that is frequently overlooked.
The odour of trichomoniasis tends to be more pungent and persistent than BV and is less reliably triggered by specific events like menstruation or intercourse. If you notice a strong, consistent, somewhat foul odour alongside a frothy or discoloured discharge, please see your gynaecologist promptly and request a full STI screen.
4. A Forgotten Foreign Body: The Cause No One Mentions
This one tends to make people uncomfortable when they first hear it, but it is clinically real, more common than most people realise, and important enough to include here.
Retained foreign bodies in the vagina, most often a forgotten tampon, a contraceptive device like a pessary or diaphragm that has shifted, or occasionally a fragment of a torn condom, can produce a deeply unpleasant, putrid odour relatively quickly. The mechanism is straightforward: foreign material disrupts the vaginal microbiome, creates a surface for bacterial biofilm to develop, and, particularly with organic materials like cotton, undergoes microbial decomposition. The result is a strong, foul, and often unmistakable smell quite distinct from BV or hormonal changes.
Forgotten tampons are the most common culprit, and they happen to women of all ages. It is not a sign of carelessness. It can happen at the end of a period when bleeding is light, during a busy day, or simply because a tampon was inserted when another was already in place.
The odour from a retained foreign body is typically severe and accompanied by abnormal, often brown or greenish discharge. It will not resolve on its own. Removal, usually by a gynaecologist or GP, is required, sometimes followed by a short course of antibiotics if significant bacterial overgrowth has occurred.
If you notice a sudden, very strong, foul vaginal odour unlike anything you have experienced before, a retained foreign body should be on the list of possibilities. Do not be embarrassed to raise it. Every gynaecologist has seen this. It requires a simple examination and is entirely treatable.
5. Diet, Sweat, and the Gut-Vagina Axis
The vaginal microbiome does not operate in isolation from the rest of your body. There is growing scientific interest in what researchers are calling the gut-vagina axis, the bidirectional communication between the gut microbiome and the vaginal microbiome, and the evidence suggests that what you eat genuinely influences vaginal ecology.
Certain foods directly affect the volatile compounds your body excretes, including through vaginal secretions. Asparagus is the famous example, but it is not alone. Garlic, onions, red meat, alcohol, and highly processed foods can all alter vaginal secretions because the compounds produced during their digestion are excreted partly through bodily fluids and skin. This does not mean these foods are harmful. It means the body is doing exactly what it is supposed to.
Dehydration is also a contributing factor that is chronically underestimated. When you are consistently under-hydrated, all bodily secretions, including vaginal discharge, become more concentrated. Concentrated secretions can carry a stronger scent. This is not pathological. It is physiological. But it is worth knowing.
The gut microbiome connection is more nuanced. Research suggests that women with diverse, healthy gut microbiomes tend to have more robust vaginal Lactobacillus populations. Conversely, gut dysbiosis, an imbalance in the gut bacteria most commonly associated with a low-fibre diet, heavy antibiotic use, or chronic stress, may contribute to vaginal microbiome instability.
There is growing evidence that dietary fibre, fermented foods, and adequate hydration support both gut and vaginal microbial health, though this area of research is still evolving. If you have noticed that your vaginal odour tends to worsen after eating certain foods, drinking alcohol, or during particularly stressful periods, these connections are worth discussing with a women’s health specialist or nutritional therapist working alongside your gynaecology team.
6. Pelvic Inflammatory Disease: When Odour Signals Something Deeper
Pelvic inflammatory disease, abbreviated as PID, is an infection of the upper reproductive tract, including the uterus, fallopian tubes, and ovaries. It most commonly develops when bacteria from the vagina or cervix travel upward into these structures, often as a consequence of untreated chlamydia or gonorrhoea, or sometimes following certain gynaecological procedures.
PID does not always present with dramatic symptoms. In fact, a significant proportion of cases are described as “subclinical,” meaning they cause mild or vague symptoms that are easily dismissed or attributed to other causes. One of these can be a persistent, sometimes unusual vaginal odour, accompanied by changes in discharge that may be heavier, more yellow or green in colour, or have an unfamiliar smell.
The mechanism is straightforward: PID involves active bacterial infection within reproductive tissues. The body produces inflammatory discharge in response, and the bacteria responsible can generate odour-producing metabolic byproducts.
Other symptoms that may accompany the odour in PID include dull, aching pelvic pain (often felt low in the abdomen, bilaterally), pain during sex (dyspareunia), pain on urination, irregular bleeding, and low-grade fever. You do not need all of these to have PID. Some women have only one or two.
PID is clinically significant not because of the odour but because untreated or repeatedly treated PID can cause scarring within the fallopian tubes, which raises the risk of ectopic pregnancy and reduces fertility. It deserves prompt, accurate diagnosis and treatment with the appropriate antibiotics, typically a combination regimen.
If your odour is accompanied by any pelvic discomfort, unusual bleeding, or pain during sex, please seek a clinical assessment quickly, ideally with a gynaecologist rather than a GP, as the examination and swab testing required is more thorough.
7. Cervical and Uterine Conditions: The Causes That Often Get Missed
This final category is the one most likely to be overlooked, both in general practice and in women’s own self-assessment, and it is perhaps the most important reason to see a specialist rather than managing vaginal odour at home.
Several cervical and uterine conditions can present with odour as an early or primary symptom.
Cervical ectropion (sometimes called cervical erosion, though that term is now considered outdated) occurs when the glandular cells that normally line the inside of the cervical canal migrate to its outer surface. This is very common, particularly in women who use hormonal contraception, during pregnancy, and in adolescence. These glandular cells produce more mucus than the cells they replace, which can lead to increased discharge with a slightly different odour than usual.
Endometrial polyps are benign (non-cancerous) growths on the inner lining of the uterus. They can cause abnormal or irregular bleeding, but they can also produce a watery, sometimes odorous discharge, particularly if the polyp develops its own blood supply and sheds tissue intermittently.
Cervical polyps behave similarly, and because they protrude through the cervix, they are slightly more likely to cause a visible discharge change.
It is also necessary to address the less common but critically important possibility: abnormal vaginal odour, particularly when accompanied by irregular bleeding, watery discharge, or post-coital bleeding, can in rare cases be an early sign of cervical cancer, according to NHS clinical guidance. This is not a reason for alarm. The vast majority of women with vaginal odour do not have cancer. But it is an absolute reason to have a cervical smear up to date and to report any of these accompanying symptoms to your gynaecologist without delay.
The mechanism across these conditions is the same: abnormal tissue or abnormal bleeding provides a substrate for bacterial growth, which in turn produces odour. Treating the odour without identifying and addressing the underlying condition is, at best, ineffective and, at worst, a missed diagnostic opportunity.
In My 19 Years of Clinical Practice
In my 19 years of clinical practice, what I have seen most often is this: women who come to me about vaginal odour have already been managing it in silence for longer than they should have. Many have spent months using products that not only failed to help but actively worsened the problem by further disrupting the vaginal microbiome. Some have been given antibiotics for recurrent BV without anyone investigating why the BV keeps returning. A few have been told, in various degrees of bluntness, that they simply need to wash more carefully. And by the time they arrive at my consulting room, there is a layer of embarrassment and self-blame sitting on top of a straightforward clinical problem.
The most counterintuitive truth I share with patients is that the vagina works best when left largely alone. The instinct to clean, neutralise, and deodorise is entirely understandable, but it is almost always working against the body’s own highly effective self-regulation. I have seen BV clear completely once a patient simply stopped using scented products and douching, without antibiotics at all, because removing the disruptive agent was enough for the Lactobacillus population to re-establish itself.
As I have seen with many patients, odour that cycles with the menstrual period, worsens around ovulation, or appears after a new sexual partner is almost never a hygiene problem. It is your microbiome responding to a shift. That shift can be identified. It can be addressed. And the conversation deserves to happen in a clinical setting, not in the shower with a bottle of something floral.
You are not the problem. Your body is trying to tell you something. The question is simply whether anyone is helping you listen.
When to See a Specialist: Specific Red Flags You Should Not Ignore
Vaginal odour on its own, particularly if mild and cyclical, may be worth monitoring rather than immediately treating. But there are specific scenarios that warrant prompt clinical attention. Here is when to act, and who to see.
If the odour is accompanied by a grey, white, or frothy yellow-green discharge and has lasted more than one week, book an appointment with your gynaecologist. Request a high vaginal swab and a specific test for both BV and Trichomonas vaginalis. Do not accept reassurance without a swab result.
If you notice the odour after missing a tampon, or if you have any doubt about whether a tampon was removed, see your GP or a gynaecologist within 24 to 48 hours. A retained foreign body can cause a significant infection relatively quickly and should not be left to resolve on its own.
If the odour is accompanied by pelvic pain, pain during or after sex, irregular bleeding, or a low-grade fever that has persisted for more than three to four days, see a gynaecologist as a matter of urgency and specifically raise the possibility of pelvic inflammatory disease. This is not an emergency in most cases, but it should not wait weeks for a routine appointment. Request an urgent referral if needed.
If you are perimenopausal or postmenopausal and have noticed a new or worsening vaginal odour alongside dryness, burning, or discomfort, ask your GP for a referral to a gynaecologist or menopause specialist with experience in genitourinary syndrome of menopause. This is a treatable condition and has specific evidence-based options, including topical oestrogen therapy, that can restore both vaginal health and quality of life significantly.
If your odour is accompanied by watery, blood-tinged, or post-coital discharge, and particularly if your cervical smear is overdue, book a gynaecology appointment and raise both concerns in the same consultation. Ensure your smear is updated and that any abnormal cells or cervical changes are examined. The combination of these symptoms together warrants investigation, not observation.
If BV has recurred three or more times in a twelve-month period, ask your gynaecologist for a referral to a specialist in vaginal microbiome health or an infectious disease specialist. Recurrent BV is a recognised clinical pattern with specific management pathways, including extended antibiotic regimens and microbiome-targeted interventions, and it should not simply be treated repeatedly with the same course of antibiotics without further assessment.
The most important principle here is precision. You deserve to understand not just that something is wrong, but specifically what it is, why it is happening, and what the most appropriate treatment pathway looks like for your individual circumstances.
You Deserve Answers, Not Just Products
If you have read this far, you have already done something important. You have refused to accept that shame is the appropriate response to a physiological symptom.
The single most important thing to take away from this article is simple: vaginal odour is a signal from your body, and signals deserve to be decoded, not silenced. Whether the cause is a microbial imbalance, a hormonal shift, an infection, or something your body is processing from a structural change, there is a clinical name for it, a test that can identify it, and a treatment that can address it.
Your next concrete step is this: if the odour has been present for more than two weeks, has changed in character, or is accompanied by any of the symptoms described above, book an appointment with your gynaecologist this week. Not eventually. This week. Bring this article if it helps you frame the conversation. Ask for a swab. Ask for the specific tests to be named. You are entitled to answers.
And if you found this helpful, please share it with a friend who has been suffering in silence about something she assumed was her fault. It almost certainly is not.
This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before making any changes to your health or treatment plan.