8 Shocking Causes of Vaginal Odor Gynecologists Warn About
You’ve noticed something is off, and now you’re deep in a Google search spiral at 11pm, hoping no one can see your screen. We see you, and we’re not here to judge.
The truth is, vaginal odor is one of the most common concerns women bring to their gynecologist, and the causes are far more varied, and sometimes surprising, than most people realize. Some are completely harmless. Others are your body’s polite way of waving a red flag that something needs attention. The tricky part is knowing the difference.
Your vagina is home to a remarkably sophisticated ecosystem. Billions of bacteria, a carefully calibrated pH level, and a self-cleaning mechanism that most laboratories would envy all work together to keep things balanced. When something disrupts that balance, your nose is often the first to know.
This post breaks down the eight causes of vaginal odor that gynecologists most want you to understand. Not to alarm you, but to arm you with knowledge so you can stop guessing, stop reaching for every scented product on the pharmacy shelf, and start actually addressing what’s going on.

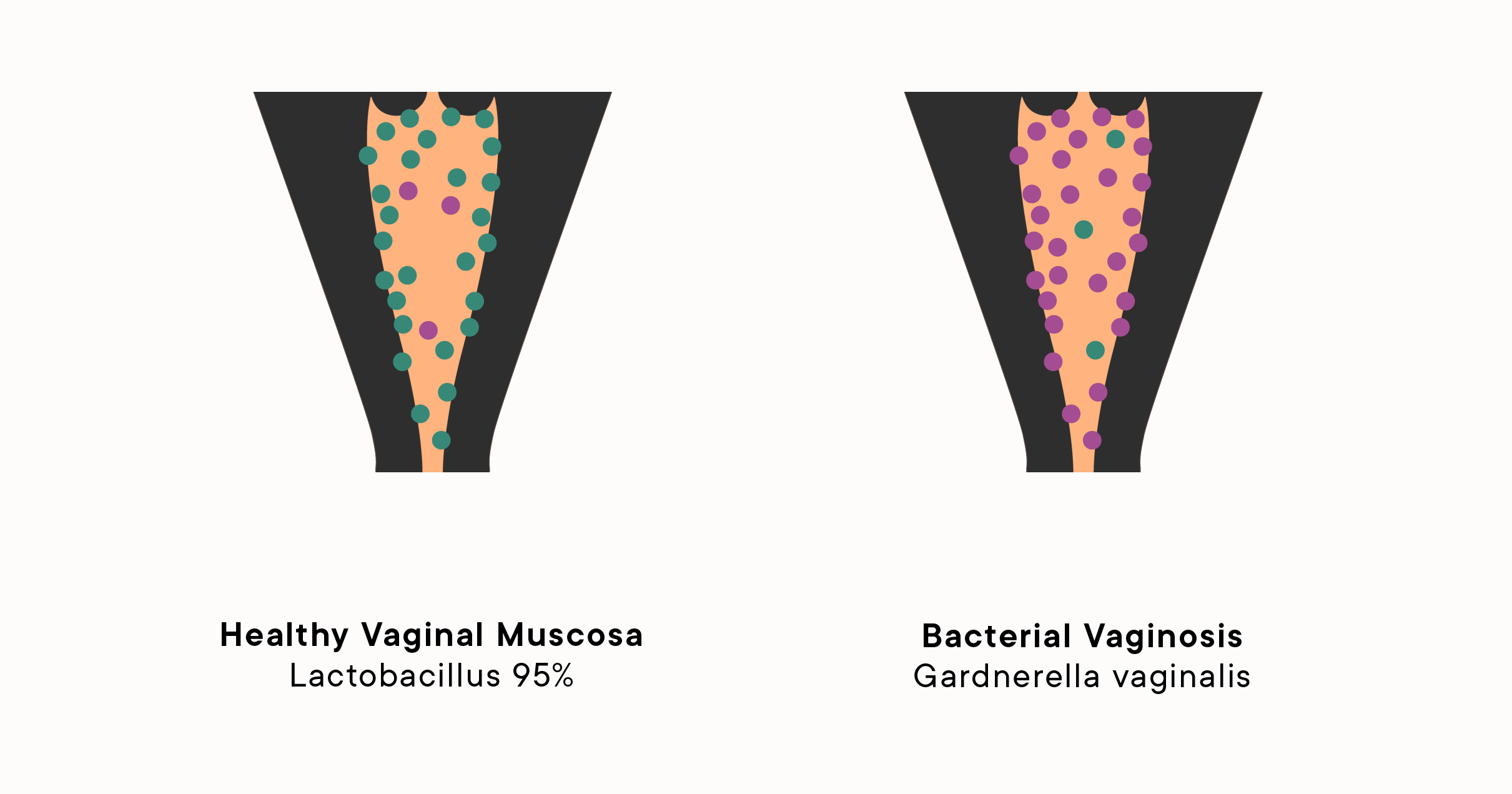
1. Bacterial Vaginosis: The Most Common Cause of Vaginal Odor Women Miss
Bacterial vaginosis, commonly called BV, is the single most frequent reason a gynecologist hears “I’ve noticed a different smell” in the exam room. BV is the most common cause of unpleasant vaginal odor in women aged 15 to 44. Yet despite how widespread it is, many women spend weeks masking the smell with products that make the problem worse.
BV happens when the balance of bacteria inside the vagina tips in the wrong direction. It occurs when there is an imbalance of the bacteria usually present in the vagina. In other words, the “bad” bacteria (anaerobes) are overpowering the “good” bacteria (lactobacilli). The result is a distinct odor that most people describe as fishy, particularly noticeable after sex.
What BV Actually Smells Like
The fishy smell associated with BV has a specific chemical explanation. Trimethylamine is the chemical compound responsible for the distinct aroma of rotting fish and some abnormal vaginal odors. “You get bacterial vaginosis when there’s an overgrowth of anaerobic bacteria in the vagina. And these anaerobic organisms are odorous.”
Alongside the odor, BV typically produces:
- Thin, watery vaginal discharge that is grayish-white in color
- Mild itching or burning, especially around the vulva
- A smell that intensifies after sexual intercourse
- Occasionally, burning when urinating
Why Women Keep Missing BV
Here is where things get counterproductive. Many women respond to the odor by douching, using feminine washes, or layering scented sprays over the problem. This is exactly the wrong move.
As gynecologist Dr. Lauren Streicher put it, treating vaginal odor with feminine washes is like washing your face and expecting bad breath to go away. BV is caused by an imbalance of bacteria inside the vagina, and feminine washes that line the shelves of pharmacies are worthless for treating it.
BV is treated with antibiotics, typically metronidazole or clindamycin, prescribed by a doctor after a proper diagnosis. It does not resolve on its own in most cases, and untreated BV can increase your risk of contracting sexually transmitted infections. If the smell is fishy and persistent, skip the pharmacy aisle and call your gynecologist.
2. Trichomoniasis: The STI Behind Vaginal Odor That People Rarely Suspect
Most women thinking about sexually transmitted infections are not thinking about their nose first. But trichomoniasis, often called “trich,” is a parasitic STI with a particularly strong and unpleasant odor as one of its hallmark symptoms.
Trichomoniasis is a sexually transmitted infection that can be treated with antibiotics. It’s known for its pungent fishy odor. “The trichomoniasis infection can be quite smelly. It’s a more pronounced fishy odor than bacterial vaginosis.”
How to Tell BV from Trichomoniasis
Both conditions produce a fishy vaginal odor, which makes self-diagnosing nearly impossible and, frankly, inadvisable. There are some differences, though.
- BV discharge is typically thin, gray, or white, and may have little to no color
- Trichomoniasis discharge is often yellow, green, or frothy, and tends to cause more irritation
- Trich frequently causes visible redness, soreness of the vulva, and pain during sex or urination
- The odor from trichomoniasis tends to be stronger and more persistent than BV
Who Gets Trichomoniasis
Trichomoniasis is actually the most common curable STI in the world, though you would not know it from how rarely it is discussed compared to chlamydia or gonorrhea. It spreads through sexual contact and can remain asymptomatic for weeks or months in some people, meaning your partner may carry it without knowing.
The treatment is a short course of antibiotics, and both partners need to be treated simultaneously to prevent reinfection. If you have a fishy vaginal odor that your doctor has already tested and ruled out BV, ask specifically to be tested for trichomoniasis.
3. A Forgotten Tampon: The Shocking Cause of Vaginal Odor Nobody Wants to Admit
This one genuinely surprises women every single time it comes up in a gynecology office, and it happens more often than you might expect. A retained tampon, meaning one that was simply forgotten during a busy or exhausted moment, is one of the most dramatic causes of vaginal odor a gynecologist encounters.
A strong rotting odor is generally due to a forgotten tampon. Although tampons cannot get completely lost inside the body, they can get stuck at the top of the vagina when forgotten and eventually emit a rotting smell.
What Actually Happens When a Tampon Is Left In
Tampons are designed to absorb moisture, which means they create a warm, damp environment that bacteria absolutely thrive in. Tampons that have been in place for more than a few hours are technically “retained,” but tampons that have been in place for days or longer are considered a potential adverse condition.
The odor that results is not subtle. Most women and their gynecologists describe it as distinctly rotten, unlike anything caused by an infection. Other symptoms to watch for include:
- Dark brown or even black discharge
- A smell that no amount of washing seems to reduce
- Mild to moderate pelvic discomfort in some cases
- Occasionally, fever if an infection has developed
What to Do If You Suspect a Forgotten Tampon
It is important to have your gynecologist do a vaginal exam if you suspect a retained tampon, as it is not always possible to detect or remove it yourself.
The good news is that removal often resolves the odor within days without the need for antibiotics, as the vagina’s natural flora rebounds quickly once the source of disruption is gone. Do not panic, but do act promptly. And if you notice a fever alongside the smell, go directly to urgent care or your doctor rather than waiting for a routine appointment.
4. Yeast Infections: When Vaginal Odor Comes With That Telltale Texture
Yeast infections are frequently discussed in the context of itching and thick discharge, but their contribution to vaginal odor is often underappreciated. The smell is different from BV, which can help distinguish the two, though many women find themselves confused between them.
A yeast infection produces a smell that is best described as yeasty, slightly sweet, or bread-like. Think fermentation, not fish. A sour odor can be normal because the natural pH of the vagina is slightly acidic, which can sometimes give off a mild sour scent. However, if the odor becomes very strong or is accompanied by other symptoms like itching, thick discharge, or irritation, it could be a sign of a yeast infection.
The Classic Yeast Infection Symptom Picture
What distinguishes a yeast infection from BV is less about the smell and more about the full constellation of symptoms:
- Thick, white, cottage-cheese-like discharge with little to no color
- Intense itching and burning around the vulva
- Redness and swelling of the vulva
- Pain during sex or urination
- A yeasty, slightly sour or bread-like odor rather than a fishy one
Why the Wrong Treatment Makes Things Worse
This is critical. Using the wrong treatment could potentially make your condition worse. Additionally, when it comes to some vaginal infections, there really is not a solid over-the-counter approach for all of them.
If you are treating a BV infection with antifungal medication (the over-the-counter yeast infection creams), you will get nowhere. The same is true in reverse. A proper gynecological exam with testing is the only reliable way to distinguish between the two and ensure you are using the right treatment.
5. Hormonal Changes: The Overlooked Cause of Shifting Vaginal Odor
Your hormones are doing enormous work behind the scenes every day, and your vaginal scent shifts right along with them. Most women notice this to some degree throughout their cycle without ever connecting the dots between their hormones and the changes they smell.
“Every woman is likely to experience some fluctuation in her vaginal odor. That’s normal and can vary throughout her menstrual cycle. Hormonal changes associated with menstruation, ovulation, and even sexual activity can all influence vaginal odor.”
When Hormonal Changes Cause More Than a Mild Shift
During pregnancy, the hormonal changes are dramatic enough that vaginal odor shifts can be quite pronounced. Increased blood flow to your vagina and changing levels of pregnancy hormones, like estrogen, progesterone and prolactin, can affect your pH level and cause new smells. Postpartum vaginal odor is common. As your uterus returns to its pre-pregnancy state, it releases blood, mucus and other debris related to pregnancy called lochia, which has a stale, metallic musty odor similar to period blood.
Menopause brings a different set of hormonal changes that affect vaginal odor in a distinct way. During menopause, estrogen levels start to decline, causing the vaginal walls to thin, which means there is less exfoliation in the vagina, and an increasing alkalinity in vaginal pH can lead to noticeable odor changes and increased infection risk.
Hormonal Odor by Life Stage
Here is a practical breakdown of what is normal at different hormonal moments:
- Ovulation: A slightly stronger, muskier smell is common mid-cycle as cervical mucus increases
- Menstruation: A metallic, iron-tinged smell from blood is completely normal
- Pregnancy: New or stronger smells due to increased blood flow and pH shifts, not always a sign of infection
- Postpartum: Lochia produces a metallic or slightly stale smell that resolves within weeks
- Perimenopause and Menopause: More alkaline pH can mean stronger odors and higher infection susceptibility
If the hormonal smell is accompanied by discharge that is green, gray, or chunky, or by significant itching or pain, that moves it from “normal hormonal fluctuation” to “time to call your doctor.”
6. Diet and Lifestyle: What You Eat Absolutely Affects Vaginal Odor
Few people draw a line between their dinner plate and what happens in their underwear the next morning, but that connection is real, documented, and a little humbling. Your diet, your hydration levels, and even your stress load can all shift how your vagina smells.
Temporary vaginal odor is common and often resolves on its own. Foods with a strong odor, like garlic or fish, can cause odor changes in your vagina. This is a direct pathway through sweat, urine, and vaginal secretions, all of which are influenced by what you consume.
The Diet-Vaginal Odor Connection
Specific dietary patterns that gynecologists and researchers have flagged as relevant include:
- Garlic, onions, and asparagus: These contain sulfur compounds that pass into sweat and secretions. Sweat can combine with vaginal discharge to make the vagina smell of strong foods, such as onions or garlic.
- High-fat diets: Some research has found a link between high-fat diets and an increased risk for odor-causing infections like bacterial vaginosis.
- High-protein and keto diets: High protein and keto diets may also be linked to a change in vaginal scent. This is partly related to how protein metabolism affects the compounds excreted through bodily fluids.
- Alcohol: Regular alcohol consumption can alter vaginal pH and contribute to a stronger smell
- Dehydration: When you are not drinking enough water, urine becomes more concentrated and ammonia-scented, which can bleed into how the entire vulvar area smells
What Actually Helps
You do not need to build your entire diet around your vagina’s preferences. But a few genuinely useful habits include:
- Staying well hydrated throughout the day
- Eating yogurt and probiotic-rich foods, which support healthy lactobacilli levels in the vagina
- Reducing highly processed and high-sugar foods, which can feed yeast overgrowth
- Not over-restricting fruits, since their natural sugars do not cause the same problems as refined sugar
7. Sweating and Poor Ventilation: The Cause of Vaginal Odor Hidden in Your Wardrobe
Here is one that is genuinely underappreciated and much easier to fix than anything involving an infection. The groin area is packed with apocrine sweat glands, the same type found in the armpits. These glands respond not just to temperature but to emotional stress, and the sweat they produce is the kind that reacts with skin bacteria to create odor.
Your body contains two types of sweat glands: apocrine and eccrine. The eccrine glands produce sweat to cool your body down, and the apocrine glands respond to your emotions. These apocrine glands populate your armpits and, your groin. When you are stressed or anxious, the apocrine glands produce a milky fluid. On its own, this fluid is odorless. But when this fluid contacts the abundance of vaginal bacteria on your vulva, it can produce a pungent aroma.
When Sweat Becomes a Problem
This type of vaginal odor tends to be muskier and more body-odor-like than infected. It gets worse with:
- Wearing tight synthetic underwear or leggings for extended periods
- Sitting for long hours without ventilation, common in sedentary desk jobs
- Intense exercise without changing out of workout clothes afterward
- High-stress periods where emotional sweat production spikes
- Hot and humid climates where the groin area stays moist throughout the day
Simple Fixes That Actually Work
This cause of vaginal odor is one of the most straightforward to manage without any medical intervention:
- Switch to breathable, 100 percent cotton underwear
- Change out of sweaty gym clothes immediately after exercise
- Sleep without underwear a few nights per week to allow ventilation
- Rinse the vulvar area with warm water after heavy sweating
- Avoid sitting in wet swimwear for extended periods
Note that the fix here is hygiene of the external area only. The vagina is self-cleaning and does not need internal washing. Using products inside the vagina to address sweat-related external odor is like taking cough medicine for a sore knee, it addresses the wrong location entirely.
8. Sexually Transmitted Infections, Pelvic Inflammatory Disease, and Rarer Causes Gynecologists Take Seriously
Beyond BV and trichomoniasis, there is a broader category of causes that gynecologists want women to stay aware of, not to create anxiety, but because early detection makes an enormous difference in outcomes.
Chlamydia and Gonorrhea
Both of these common STIs can produce vaginal discharge with an unpleasant odor, though they are less reliably associated with a strong smell than trichomoniasis. Many women with chlamydia or gonorrhea have no symptoms at all, which is exactly why regular gynecological exams are essential, because conditions like sexually transmitted infections, vulvar or vaginal cancer, fibroids, and endometriosis are conditions that could be spotted by a gynecologist even in the absence of obvious symptoms.
Pelvic Inflammatory Disease (PID)
PID is an infection of the reproductive organs that can develop when STIs are left untreated and spread upward from the vagina and cervix. Vaginal odor accompanied by pelvic pain, fever, pain during sex, or unusual discharge warrants immediate medical evaluation, not a wait-and-see approach.
Rectovaginal Fistula
This is a rare but serious condition in which an abnormal opening develops between the rectum and the vagina, usually as a result of childbirth trauma, surgery, or Crohn’s disease. It produces a very distinct fecal odor from the vaginal area that does not respond to any hygiene measures because the cause is structural, not bacterial. Surgery is typically required.
Cervical and Vaginal Cancer
Persistent vaginal odor alongside unusual bleeding, particularly between periods or after menopause, warrants prompt evaluation. While cancer is a rare cause of vaginal odor, it is one that gynecologists are trained to rule out. Per Cleveland Clinic’s guidance on vaginal health, prolonged abnormal vaginal odor accompanied by discharge, burning and itching should prompt a visit to a healthcare provider.
Poorly Controlled Diabetes
Some women with undiagnosed or poorly managed diabetes notice a sweet or fruity vaginal odor, which can be related to elevated blood sugar levels affecting vaginal secretions and increasing susceptibility to recurrent yeast infections. If you are experiencing frequent yeast infections alongside other symptoms of diabetes, like excessive thirst or fatigue, discuss this pattern with your doctor.
Quick-Reference Table: 8 Causes of Vaginal Odor at a Glance
| Cause | Typical Odor | Key Symptoms Alongside Odor | Requires Medical Treatment? | How It’s Treated |
|---|---|---|---|---|
| Bacterial Vaginosis (BV) | Fishy, especially after sex | Thin gray-white discharge, mild itching | Yes | Antibiotics (metronidazole or clindamycin) |
| Trichomoniasis | Strong fishy, more intense than BV | Green/yellow frothy discharge, irritation, soreness | Yes | Antibiotics (both partners treated) |
| Forgotten Tampon | Rotten meat, very strong | Brown/dark discharge, possible pelvic discomfort | Removal needed, sometimes antibiotics | Physical removal by gynecologist |
| Yeast Infection | Yeasty, bread-like, slightly sour | Thick white discharge, intense itching, redness | Often OTC, confirm diagnosis first | Antifungal medication |
| Hormonal Changes | Metallic, musky, or mildly sour | Varies by cycle stage, usually no discharge changes | No (if no accompanying symptoms) | No treatment needed unless infection develops |
| Diet and Lifestyle | Variable; musky, onion-like, ammonia | None typically, aside from general odor change | No | Dietary adjustment, hydration |
| Sweat and Poor Ventilation | Musky, body odor-like | Worse after exercise, heat, or stress | No | Hygiene adjustments, breathable clothing |
| STIs, PID, Rarer Causes | Variable, foul, sometimes fecal | Pelvic pain, fever, abnormal bleeding | Yes, urgently for PID/STIs | Dependent on diagnosis; antibiotics, surgery, or cancer treatment |
What to Do (and What to Absolutely Stop Doing)
Before you reach for anything in the feminine hygiene aisle, take a moment. Not everything marketed to your vagina is good for it. In fact, many products create the very problems they claim to solve.
Stop doing these things:
- Douching. Full stop. The vagina is self-cleaning, and douching strips the healthy bacteria that protect it, raising your BV and yeast infection risk significantly
- Using scented soaps, gels, or sprays inside or directly at the vaginal opening
- Assuming the odor will resolve without intervention when it has persisted longer than a week or is accompanied by other symptoms
- Self-diagnosing and self-treating without knowing which condition you actually have
Start doing these things:
- Wash only the external vulvar area with warm water and, if desired, a mild unscented soap
- See a gynecologist if the odor is persistent, strong, or accompanied by discharge changes, itching, pain, or burning
- Use condoms consistently to protect your vaginal pH and reduce STI risk
- According to the American College of Obstetricians and Gynecologists, women should seek care when vaginal symptoms are new, unusual, or recurring, rather than repeatedly self-treating without a confirmed diagnosis
- Keep up with routine gynecological exams even when you feel fine
The Bottom Line on Vaginal Odor Causes
Your vagina is not supposed to smell like roses, fresh linen, or a tropical beach. It is supposed to smell like a vagina, which is to say mildly, naturally, and uniquely yours. The problem only begins when something upsets the ecosystem.
What gynecologists most want women to understand is this: vaginal odor is almost never something to be ashamed of, but it is always worth paying attention to. Your body communicates through symptoms, and a change in smell is one of the clearest signals it has. The good news is that nearly every cause on this list is treatable, and most are treatable quickly.
Do not spend months masking a smell that could be resolved in days with the right diagnosis and treatment. You deserve actual answers, not a prettier problem.
Still Have Questions? Here’s What to Do Next
If you found this helpful, share it with a friend who deserves to actually understand what is going on with their body, because this information is too important to stay hidden in a late-night search history.
Read Next:
- What Your Vaginal Discharge Color Is Actually Telling You
- Why Recurring BV Keeps Coming Back (And How to Finally Stop the Cycle)
- The Truth About Probiotics and Vaginal Health
Drop a comment below: Have you ever been surprised by the cause of a vaginal odor change? What helped most? Sharing your experience might be exactly what another woman needs to read tonight.
This article is for informational purposes only and is not a substitute for professional medical advice. If you are experiencing persistent vaginal odor or any of the symptoms described, please consult a licensed gynecologist or healthcare provider.