

Painful Sex After Baby: 7 Honest Reasons No One Warned You About (And 5 Powerful Fixes That Actually Help)
By Dr. Naomi, Board-Certified Women’s Health Physician, Reproductive Endocrinology & Integrative Gynaecology
You Googled This at 2am. Let’s Talk Honestly.
You waited the full six weeks.
You had the check-up. Your GP looked up from the notes, said “everything looks fine,” and signed you off. So you tried. And it hurt. Maybe it burned. Maybe it felt like tearing. Maybe it just felt completely, utterly wrong.
Nobody told you it would be like this. The antenatal classes skipped it. The baby books glossed over it. Your midwife mentioned it in passing, offered you a tube of lubricant, and moved on to discussing your stitches.
And now you’re lying awake at 3am wondering if your body will ever feel like yours again.
Here is the most important thing I want you to hear first: painful sex after having a baby is extraordinarily common, it has real, treatable clinical causes, and your experience is not a failure. It is not a sign your relationship is in trouble. It is not something you simply have to endure.
It is a medical issue. And it deserves a medical answer.
This article is that answer.
What Painful Sex After Baby Actually Is (And Why Your Six-Week Check Missed It)
The clinical term is postpartum dyspareunia, meaning painful sexual intercourse occurring in the period following childbirth. “Dyspareunia” simply means pain during sex, and “postpartum” refers to the period after delivery.
Think of your pelvic floor and vaginal tissues like a complex suspension bridge. Pregnancy stretches the cables, shifts the load, and alters the tension on every component. Labour and delivery, whether vaginal or by caesarean, then ask that bridge to handle a seismic event. Restoring normal function after that takes far more than six weeks and a quick visual inspection.
Here is the important clinical reality: postpartum dyspareunia is significantly underdiagnosed and undertreated, primarily because most routine six-week postnatal appointments are brief, symptom-focused, and rarely include an internal pelvic examination. Research published in gynaecological literature consistently suggests that between 40% and 60% of women experience some form of painful sex in the first three months after delivery, yet the majority never receive a formal diagnosis or targeted treatment plan.
It matters because untreated postpartum dyspareunia does not always resolve on its own. For some women it does. For many others, without the right support, it becomes a persistent problem that affects relationships, self-esteem, and quality of life for months or years.
The featured snippet answer: Postpartum dyspareunia is persistent or recurring pain during sexual intercourse following childbirth. It affects up to 60% of new mothers and is caused by a combination of hormonal shifts, tissue trauma, pelvic floor dysfunction, and psychological factors. Most cases are treatable with the right clinical support, though they are frequently missed at routine postnatal check-ups.
You deserve to know what is actually happening in your body. So let us go through it, honestly and completely.
Part One: 7 Honest Reasons Painful Sex After Baby Happens (That No One Warned You About)
Reason 1: Oestrogen Has Left the Building (And It Has Taken Your Vaginal Comfort With It)
This is the single most common cause of painful sex after baby, and it is almost never explained clearly at the postnatal appointment.
During pregnancy, your oestrogen levels are extraordinarily high, keeping vaginal tissues well-lubricated, elastic, and healthy. After delivery, oestrogen drops sharply. If you are breastfeeding, it drops even further, because prolactin (the hormone that drives milk production) actively suppresses oestrogen production. This is not a flaw in your body’s design. It is a deliberate physiological mechanism. But the consequence, for many women, is that vaginal tissues become thinner, drier, and far more sensitive to friction.
Clinically, this is called hypoestrogenic vaginal atrophy, meaning the vaginal walls thin out and lose their natural moisture in response to low oestrogen. During penetration, this thinned tissue experiences micro-trauma, leading to burning, soreness, and sometimes bleeding after sex.
The mechanism is straightforward: oestrogen maintains the glycogen content of vaginal epithelial cells, which feeds the healthy lactobacillus bacteria that keep tissues supple. Without adequate oestrogen, this protective cycle breaks down. The result is tissue that is physiologically more similar to post-menopausal vaginal tissue than the tissue you had before pregnancy.
This is why the lubricant your midwife handed you may not be enough. Lubricant addresses surface friction. It does not address the underlying tissue health.
For breastfeeding mothers especially, this low-oestrogen state can persist for the entire duration of nursing, which means painful sex is not a “just for the first few weeks” issue. It can continue for months. That is not unusual, and it is not permanent.
Reason 2: Your Pelvic Floor Is Either Too Tight or Too Weak (And Either Can Cause Pain)
Most women have heard they should do pelvic floor exercises after birth. Far fewer are told that doing too many, or doing them when the pelvic floor is already in a state of tension, can make things significantly worse.
Here is what most postnatal advice misses: the pelvic floor can fail in two completely opposite directions.
The first is pelvic floor weakness, where the muscles have been overstretched during labour and delivery, losing the tone and coordination needed to support the vaginal walls during sex. This can cause a sensation of collapse, discomfort from lack of support, and a feeling of “looseness” that is actually the muscles failing to engage correctly.
The second, and far less discussed, is hypertonic pelvic floor dysfunction, where the muscles go into a state of chronic bracing or spasm following the trauma of birth. This is involuntary. Your body, having experienced something physically overwhelming, keeps the pelvic floor in a state of protective contraction. During penetration, instead of the muscles gently yielding, they resist. The result is a sharp, burning, or tearing sensation that has nothing to do with lubricant.
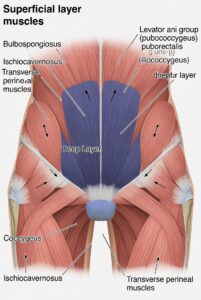
The clinical mechanism here involves the levator ani muscle group, a sling of muscles running from the pubic bone to the coccyx that forms the base of the pelvis. After a difficult or prolonged labour, instrumental delivery (forceps or ventouse), or significant perineal tearing, these muscles can develop trigger points and restrict normal movement.
Critically, doing aggressive Kegel exercises when you have a hypertonic pelvic floor is counterproductive. It would be like treating a cramped muscle by asking it to contract harder. This is why a specialist assessment from a pelvic floor physiotherapist is not a luxury. It is a clinical necessity.
Reason 3: Scar Tissue from Tears or Episiotomy Is Changing How Everything Moves
If you had a perineal tear during delivery, whether that was a first-degree graze or a more significant third- or fourth-degree tear, or if you had an episiotomy (a surgical cut made to widen the vaginal opening during delivery), you have scar tissue.
Scar tissue is not inherently problematic. It is your body’s method of repair. But scar tissue is structurally different from the original tissue it replaces. It is less elastic, less well-vascularised (meaning it has a reduced blood supply), and it tends to be denser and more adhesive than normal tissue.
During sex, where vaginal and perineal tissues need to stretch and move freely, scar tissue that has not been properly mobilised can pull, catch, and tear. The technical term is tethered scar adhesions, where the healed tissue has attached to underlying structures and restricts normal movement. You may feel a sharp, specific pain at one particular point of penetration, rather than a diffuse burning.
What makes this especially frustrating is that scar tissue can look completely healed externally. A GP doing a visual check at six weeks may see nothing unusual. But internally, the adhesions are still limiting mobility.
The good news is that scar tissue responds very well to targeted massage and manual therapy when performed by a qualified pelvic physiotherapist. It is not a permanent sentence. But it does require active, specific treatment, not just time.
Reason 4: Vaginal Microbiome Disruption Is Creating Inflammation You Cannot See
This is one of the most under-discussed contributors to postpartum sexual discomfort, and it is almost never raised in routine postnatal care.
Your vaginal microbiome is a carefully balanced ecosystem of bacteria, predominantly lactobacillus species, that maintain an acidic pH and protect the vaginal mucosa from irritation and infection. During pregnancy, this ecosystem is typically in excellent condition. Oestrogen keeps it stable and the dominant lactobacillus strains flourish.
After birth, several things happen simultaneously. Oestrogen falls (as discussed), which reduces glycogen availability for lactobacillus. Lochia (postpartum bleeding and discharge) alters the vaginal pH for several weeks. Antibiotics prescribed during or after labour, which are very commonly used in caesarean births and in cases of prolonged rupture of membranes, can further deplete the healthy bacterial community.
When lactobacillus populations fall, opportunistic species move in. This creates what is called vaginal dysbiosis, an imbalance in the microbial community. Even without a diagnosable infection, this dysbiosis creates a low-grade inflammatory environment in the vaginal tissue. That inflammation translates directly into heightened sensitivity, irritation, and pain during sex.
You may not have a full-blown bacterial vaginosis (BV) infection. Your swab may come back “negative.” But sub-clinical dysbiosis can still cause significant discomfort. The symptom that most commonly points to this cause is a persistent burning or rawness that seems unrelated to dryness, and that may be accompanied by an altered or unfamiliar vaginal odour even without a confirmed infection.
Reason 5: Provoked Vestibulodynia: The Pain Condition Most GPs Have Never Heard Of
This one deserves its own section because it is genuinely underdiagnosed, underserved in mainstream medicine, and affects a meaningful proportion of women who experience persistent postpartum sexual pain.
Vestibulodynia is pain localised to the vulvar vestibule, the small ring of tissue at the entrance to the vagina, where the inner labia minora meet the vaginal opening. “Provoked” means the pain is triggered by contact or pressure (as opposed to spontaneous pain that occurs unprovoked). The most common trigger is attempted penetration during sex.
The sensation is typically described as a sharp, burning, or stinging pain at the vaginal entrance, sometimes likened to “a paper cut” or “rubbing sandpaper.” It can occur with any form of penetration, including tampon use and gynaecological examinations.
Provoked vestibulodynia exists prior to pregnancy in some women, but it can also be triggered or significantly worsened by the hormonal and tissue changes of the postpartum period. Specifically, oestrogen receptors in the vestibular tissue become sensitised in a low-oestrogen environment, and nociceptors (pain nerve fibres) in this area can become upregulated, meaning they fire in response to stimuli that would not normally be painful.
The clinical mechanism involves a combination of peripheral sensitisation (an increase in pain signalling from the local nerve endings) and, in chronic cases, central sensitisation (where the brain begins to amplify pain signals from the pelvic region more broadly).
The reason this is so frequently missed is simple: most GPs are not trained to examine for it, and many women describe the symptom vaguely as “pain during sex,” which is attributed to dryness and addressed with lubricant. A proper diagnosis requires a specific examination technique called the Q-tip test, where light pressure is applied to different points around the vestibule to map the precise location and severity of pain. Most routine postnatal appointments do not include this assessment.
Reason 6: A Caesarean Section Does Not Protect You From Pelvic Pain (And Here Is Why)
There is a widespread assumption, even among some healthcare providers, that if you delivered by caesarean section, you will be spared postpartum sexual pain. This is not accurate, and believing it can leave C-section mothers without the assessment or support they need.
Here is what actually happens. Even if you never experienced labour, pregnancy itself alters the pelvic floor. The weight of a growing uterus, the hormonal changes that soften connective tissue throughout the pelvis (particularly the hormone relaxin), and the shifts in posture and biomechanics across nine months all affect pelvic floor function regardless of delivery mode.
But the caesarean scar itself introduces a specific problem: internal scar adhesions. The surgical repair of the uterus, the fascia (connective tissue), and the abdominal wall layers can create adhesions, bands of fibrous tissue that attach structures that should move independently of each other.
These adhesions can tether the bladder, the uterus, or the anterior vaginal wall in ways that restrict normal movement during sex. They can also affect the nerves of the lower pelvis and cause referred pain into the vagina, even though the scar is at the bikini line.
Additionally, many women who deliver by caesarean section following a prolonged or difficult labour have already experienced significant pelvic floor strain during the labour process itself, prior to the surgical delivery. This means they may carry both the effects of labour-related pelvic floor stress and the consequences of surgical adhesions.
If you had a C-section and still experience pain during sex, it is entirely valid and it warrants a full clinical assessment. Do not let anyone tell you it is unexpected.
Reason 7: Your Nervous System Is Still on High Alert from the Birth Experience
This is perhaps the least-discussed reason of all, and it is the one I see dismissed most often. But the evidence is increasingly clear, and the clinical reality is something I encounter regularly.
Childbirth is a major physiological and psychological event. For many women, it is a positive one. For others, it involves elements of fear, pain, loss of control, unexpected intervention, or outright trauma. The distinction between a “difficult birth” and a “traumatic birth” is not always obvious from the outside, and it is intensely subjective.
What we know from research into birth-related PTSD and pelvic pain is that psychological trauma from labour can translate directly into physical pain during sex. The mechanism involves the autonomic nervous system. Following a traumatic experience, the nervous system can become stuck in a state of threat response, where the body reflexively braces, tenses, or recoils in anticipation of harm.
In the pelvis, this manifests as the pelvic floor muscles contracting involuntarily during any form of sexual contact, a condition sometimes called vaginismus. This is not a conscious choice. It is your nervous system trying to protect you.
Beyond frank trauma, many new mothers experience profound changes in their sense of bodily ownership and identity after birth. The body has done something extraordinary and also, in many cases, something painful and undignified. Reconnecting with your body as a site of pleasure, rather than merely a site of function and recovery, takes time and often requires active support.
Research in psychosexual medicine consistently shows that fear of pain itself, once pain has been experienced, triggers a feedback loop in which the anticipation of pain causes muscle tension, which causes pain, which reinforces fear. This is not a weakness. It is neuroscience.
Understanding this cause does not mean the pain is “all in your head.” It means your head and your body are connected, and treating the physical causes alone is sometimes not sufficient.
Part Two: 5 Evidence-Based Fixes That Actually Help
Fix 1: Pelvic Floor Physiotherapy, The Single Most Effective Starting Point
Mechanism: A specialist pelvic floor physiotherapist conducts a thorough internal and external assessment of muscle tone, coordination, and tissue mobility. Depending on what they find, treatment may include manual therapy to release trigger points and hypertonic muscles, graduated internal stretching exercises to restore mobility, neuromuscular retraining to improve coordination between muscle groups, scar tissue mobilisation for perineal or caesarean scars, and specific relaxation techniques for hypertonic dysfunction.
Evidence level: Clinical consensus among urogynaecology and obstetric physiotherapy bodies is strong and consistent. Multiple systematic reviews and clinical guidelines, including those from the Chartered Society of Physiotherapy in the UK, support pelvic floor physiotherapy as a first-line intervention for postpartum dyspareunia. The NHS guidance on perineal care and recovery acknowledges physiotherapy as a core component of postpartum recovery, though access through primary care varies considerably.
Practical implementation: Ask your GP for a referral to a women’s health physiotherapist. If NHS waiting times are lengthy, independent pelvic floor physiotherapists practise privately across the UK and will typically conduct an initial assessment followed by a structured treatment plan over six to twelve weeks. The number of sessions required varies by cause and severity, but most women with straightforward postpartum dyspareunia see meaningful improvement within four to eight sessions of targeted therapy.
The critical practical note: be honest with your physiotherapist about exactly where the pain occurs, what type of sensation it is, and whether it is getting better or worse over time. Precision in symptom description leads to precision in treatment.
Fix 2: Topical Oestrogen Therapy, Safe, Effective, and Significantly Underused
Mechanism: Low-dose vaginal oestrogen is applied directly to vaginal and vulvar tissues in the form of a cream, a small tablet (pessary), or a ring device. Unlike systemic hormone replacement therapy, topical vaginal oestrogen is delivered locally with minimal absorption into the bloodstream. It works by restoring oestrogen receptor activity in vaginal epithelial cells, which in turn increases the natural production of vaginal moisture, improves tissue thickness and elasticity, lowers vaginal pH back toward its healthy acidic range, and reduces the inflammatory sensitivity of vulvar nerve endings.
Evidence level: The evidence for low-dose vaginal oestrogen in treating hypoestrogenic dyspareunia is exceptionally strong. Clinical consensus among the British Menopause Society, ACOG, and gynaecological organisations worldwide supports its use. Importantly, safety studies have consistently shown that low-dose vaginal oestrogen does not meaningfully raise systemic oestrogen levels, making it generally safe even for breastfeeding mothers, though this should always be discussed with your prescribing physician.
Practical implementation: You will need a prescription from your GP or gynaecologist. The most common preparation used in the UK is a low-dose oestradiol cream or vaginal pessary applied two to three times per week. Effects are not immediate: most women notice improvements in tissue comfort within four to six weeks of consistent use, with full benefit typically achieved at eight to twelve weeks. Using it alongside a good-quality vaginal moisturiser (applied regularly between applications) and a water-based lubricant during sex will typically produce the most complete symptom relief.
It is worth noting that many women are unnecessarily cautious about vaginal oestrogen because of historical concerns about oestrogen therapy more broadly. Those concerns relate primarily to systemic, oral oestrogen therapy, not to the low-dose topical application discussed here. Do not let generalised worry prevent you from accessing a treatment that has an excellent safety profile and excellent outcomes.
Fix 3: Vaginal Moisturisers and Targeted Lubricants, There Is a Clinical Difference Between the Two
Mechanism: This matters more than most people realise, because moisturisers and lubricants do different things and should be used differently.
A vaginal moisturiser is not a lubricant. It is a product designed to be used regularly (typically two to three times per week, not just before sex) to restore and maintain hydration in vaginal tissues over time. Effective vaginal moisturisers typically contain either hyaluronic acid, which has been shown in clinical trials to match or approach the efficacy of low-dose vaginal oestrogen for mild-to-moderate atrophic symptoms in some women, or a polycarbophil-based formulation that adheres to vaginal walls and provides sustained moisture.
A lubricant is used during sexual activity to reduce friction at the point of contact. Water-based lubricants are the most widely recommended for general use and are safe with all contraceptives. Silicone-based lubricants are longer-lasting and may be preferable when dryness is more severe, though they are not safe with silicone sex toys. Avoid lubricants containing glycerin, fragrance, or warming or cooling additives, as these can disrupt vaginal pH and trigger irritation in already-sensitive tissue.
Evidence level: The evidence for hyaluronic acid vaginal moisturisers is growing. Research suggests that in women with hypoestrogenic vaginal symptoms, hyaluronic acid preparations can provide meaningful relief and may be a useful option for women who prefer to avoid hormonal therapy entirely. Clinical consensus holds that using both a regular moisturiser and a quality lubricant simultaneously produces better outcomes than either alone.
Practical implementation: Use the moisturiser consistently on a routine schedule, independent of sexual activity. Think of it like a daily skin moisturiser rather than something you reach for only when you need it. Use the lubricant generously during sex. Apply it before penetration, not as an afterthought once discomfort has already begun.
Fix 4: Scar Tissue Massage and Desensitisation, Targeted and Learnable
Mechanism: Scar tissue, whether from perineal tears, episiotomies, or caesarean incisions, responds to regular mechanical loading and massage by gradually remodelling. The collagen fibres within a scar, initially laid down in a disorganised pattern during healing, can be encouraged to realign more closely with normal tissue through consistent, controlled pressure and movement. This reduces the tethering and pulling sensation and restores more normal tissue mobility.
For perineal scar tissue, a technique called perineal massage involves applying gentle sustained pressure to the scar itself and the surrounding tissues to increase pliability. For caesarean scar tissue, a similar technique applied to the abdominal scar can help reduce the deep internal adhesions that contribute to pelvic pain.
Evidence level: There is growing evidence that perineal scar massage begun around six to eight weeks postpartum, once the wound has closed, improves scar tissue mobility and reduces associated pain. Clinical guidance from pelvic floor physiotherapy bodies supports its use as part of a broader postpartum recovery programme. The evidence base for caesarean scar massage is still building, but clinical experience strongly supports its benefit and it carries no meaningful risk.
Practical implementation: Most women benefit from being taught this technique by their pelvic floor physiotherapist first, rather than attempting it alone based on a video or written guide. The location, direction, and pressure of massage matter, and starting with professional guidance reduces the risk of doing it incorrectly. Once you have been shown the technique, it can typically be self-administered at home on a daily or every-other-day basis.
Do not begin perineal massage before your scar has fully closed, typically no earlier than six weeks postpartum and only once all visible wound healing is complete. Introduce the pressure gradually. You should feel a stretching sensation, not sharp pain.
Fix 5: Psychosexual Support and Addressing the Nervous System Component
Mechanism: When fear of pain, birth-related trauma, or anxiety is contributing to sexual pain, addressing the psychological component is not an optional extra. It is a clinical intervention in its own right.
Psychosexual therapy, delivered by a qualified therapist with specific training in sexual dysfunction and women’s health, works through several mechanisms. It provides a framework for understanding how trauma or anxiety has altered your neurological response to intimacy. It delivers cognitive tools to interrupt the fear-pain-tension cycle. It includes graduated sensate focus exercises, a programme of progressive, non-goal-oriented physical intimacy designed to rebuild comfort and trust with your body. And it opens the communication between partners in a structured, guided way, which is important because unspoken fear and pressure from either partner amplify pain.
Evidence level: Clinical consensus from psychosexual medicine bodies and the British Society for Sexual Medicine supports psychosexual therapy as an evidence-based treatment for dyspareunia with a significant psychological component. Research on the integration of psychological and physical treatment approaches, sometimes called a biopsychosocial model, consistently shows better outcomes than treating either dimension in isolation.
Practical implementation: You can ask your GP for a referral to a psychosexual therapist through NHS sexual health services, or seek a private therapist via the College of Sexual and Relationship Therapists (COSRT), the UK’s leading accrediting body for this specialty.
You do not need to have experienced a formally traumatic birth to benefit from this support. If sex feels emotionally loaded, if you are dreading rather than desiring intimacy, or if the anticipation of pain has begun to shape how you feel about your body, this kind of support is appropriate and valuable.
It can also be enormously helpful for your partner to be involved in at least some sessions, not because the problem is theirs to fix, but because shared understanding changes the dynamic in the bedroom more profoundly than anything either of you can do individually.
In My 19 Years of Clinical Practice
In my 19 years of clinical practice, what I’ve seen most often is a woman sitting in front of me who has been experiencing painful sex for six, nine, sometimes eighteen months after her baby was born, and who was told at her six-week check that everything was fine. She has been waiting for it to resolve on its own because no one gave her permission to ask for more help. She is often exhausted, often quietly distressed about the impact on her relationship, and almost always carrying some version of the belief that this is simply what motherhood does to you, that this is a sacrifice you accept. And when I explain the actual clinical reasons behind her pain, things like hypertonic pelvic floor, or vestibulodynia, or low-dose vaginal oestrogen, I watch her face shift from resignation to something closer to relief. The problem had a name. The problem had a cause. And most importantly, the problem had a solution. The tragedy is not that these conditions exist. Bodies are complicated, and birth is demanding. The tragedy is that so many women wait so long to get answers because no one asked them the right questions in the first place.
When to See a Specialist: Specific Signs That Need Clinical Assessment
Do not wait indefinitely for painful sex after baby to resolve by itself. There are clear signs that warrant prompt or urgent specialist review.
If you experience sharp, localised pain at the vaginal entrance with any form of penetration that has persisted for more than eight weeks postpartum, request a referral to a gynaecologist or, ideally, a vulval specialist or a clinic with expertise in vestibulodynia. Ask specifically for a vestibular examination and Q-tip test.
If your pain is accompanied by persistent burning, rawness, or an abnormal discharge that has not been resolved by treatment for infection, ask your GP for a referral to a gynaecologist for assessment of vaginal atrophy and microbiome evaluation.
If you have significant perineal scarring, pain at the site of a repair, or visible deformity at the perineum beyond twelve weeks postpartum, ask for a referral to a urogynaecologist or pelvic floor physiotherapist with specialist training in scar assessment.
If you are experiencing pain you believe may be related to your caesarean scar, including pain deep in the pelvis or lower abdomen during sex, a urogynaecologist or pelvic pain specialist can assess for internal adhesions.
If you are experiencing significant anxiety, avoidance of intimacy, or symptoms consistent with birth-related PTSD, including flashbacks, hypervigilance, or emotional numbness, please seek a referral to a psychosexual therapist or a perinatal mental health service. The pain you feel in your body is real, and so is the pain you feel in your mind. Both deserve care.
If you are breastfeeding and experiencing vaginal atrophy symptoms, ask your GP or midwife about low-dose topical oestrogen therapy. This conversation often does not happen unless you initiate it.
You Are Not Broken. You Are Under-Supported.
Your body carried and delivered a human being. That is extraordinary. It is also physically significant in ways that our postnatal care system does not always fully acknowledge or address.
The most important thing I want you to take from this article is this: painful sex after baby is a clinical problem with clinical solutions. It is not a life sentence. It is not a sign your relationship is failing. It is not simply what motherhood costs.
The single most valuable next step you can take today is to go back to your GP, name your symptom clearly, and ask for a referral to a pelvic floor physiotherapist. That one appointment can unlock an entire pathway of care that the standard postnatal check never opened.
As I’ve seen with many patients, that moment of finally asking is the turning point. Not because the therapy is instant, but because having someone genuinely assess what is happening, name it, and offer a plan changes everything about how you carry it.
You do not have to stay quiet about this. Your comfort matters. Your pleasure matters. Your recovery matters.
Share this article with a new mum who needs to hear that her experience is real, her pain is explainable, and help is available.
Or, if you are ready to learn more, read next: How to Talk to Your Doctor About Pelvic Floor Problems (Without Being Dismissed)
This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before making any changes to your health or treatment plan.