

What No One Tells You About Miscarriage: 10 Devastating Truths and the 3 Hopeful Facts That Can Change Everything
The 2am Search You Hoped You’d Never Make
You are lying awake, phone screen bright in the dark. You have typed “is it normal to feel this empty after a miscarriage” and you are waiting for something — anything — that sounds like it was written for you, not for a textbook.
Maybe it happened last week. Maybe it happened two years ago and it still sits in you like a stone. Maybe you had one brief, heart-shattering appointment where a doctor used the word “products of conception” and you wanted to say: that was my baby.
Perhaps no one told you that you might grieve for months. Perhaps someone told you to “just try again” as though the pregnancy you lost was a failed exam, not a person you had already started imagining. Perhaps you have never spoken about it out loud — not fully — because you were not quite sure you were allowed to.
You are allowed to.
This article is for you — for every woman who has experienced pregnancy loss and found that the clinical answers barely touched the edges of what she was actually living. What follows are the truths that mainstream medicine often sidesteps, and the three evidence-grounded reasons to hold on to genuine hope.
Understanding Miscarriage: The Clinical Foundation
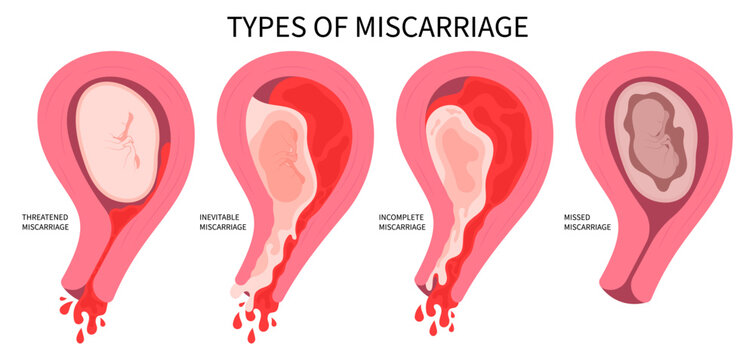
Miscarriage — medically termed spontaneous abortion — is the loss of a pregnancy before 24 weeks of gestation, most often occurring within the first 12 weeks. It is the most common complication of early pregnancy.
Think of early fetal development as an extraordinarily complex, precisely timed construction project. Chromosomes must pair correctly, hormones must signal at precise intervals, the uterine lining must be receptive, and implantation must be deep enough to sustain growth. When any one of those variables is disrupted, the body often ends the pregnancy before the problem compounds. It is not a failure. It is, in many cases, the body responding with remarkable biological intelligence to a situation that could not continue safely.
Yet despite being this common, miscarriage remains profoundly underserved in mainstream medicine. Most women receive a diagnosis, possibly a management plan, and very little else. The emotional sequelae — which clinical research consistently shows can resemble post-traumatic stress disorder in intensity — are rarely addressed systematically. The physiological complexity beneath each individual loss is rarely investigated until a third miscarriage has occurred. That gap between what women need and what they receive is precisely what this article aims to bridge.
10 Miscarriage Truths Most Women Are Never Told
1. Chromosomal abnormality is the cause in most first-trimester losses — and it is almost never your fault
Research consistently indicates that between 50 and 70 per cent of first-trimester miscarriages involve a chromosomal abnormality in the embryo — typically an error that occurred during the formation of the egg or sperm, or during the very first cell divisions after fertilisation. These are called de novo errors, meaning they arise spontaneously rather than being inherited.
Nothing you ate, how much you exercised, whether you had a stressful week, or whether you lifted something heavy caused your miscarriage. For the majority of first-trimester losses, the embryo had an error that made a continuing pregnancy incompatible with life. The body recognised this. The body responded accordingly.
This truth matters not as a consolation prize, but as a clinical fact that deserves to be said clearly and early in every consultation.
2. Recurrent miscarriage is more common than the statistics suggest — and “unexplained” does not mean untreatable
Clinical consensus defines recurrent miscarriage as the loss of three or more consecutive pregnancies. Studies suggest this affects approximately 1 per cent of couples trying to conceive. However, growing evidence suggests that two losses in a row — particularly in women over 35 — warrant investigation rather than reassurance, and many reproductive medicine specialists now advocate investigating after two losses regardless of age.
“Unexplained recurrent miscarriage” is a label applied to roughly 50 per cent of recurrent miscarriage cases after standard testing. The word “unexplained” can feel like a door closing. It should not. It means that the cause has not yet been identified with current standard testing — not that no cause exists, and not that treatment cannot help. Emerging research into uterine natural killer cells, endometrial receptivity, and coagulation pathways is actively changing what “unexplained” means.
3. Your period after miscarriage is not simply your cycle resuming — it is physiologically complex
Most women are told to expect their menstrual cycle to return within four to six weeks of a miscarriage. What they are rarely told is that the first several cycles following pregnancy loss can be irregular, heavier, or more painful than their previous baseline — and that this is expected and typically temporary.
The hormonal recalibration following pregnancy loss takes time. Beta-human chorionic gonadotropin (beta-hCG) — the pregnancy hormone — does not drop to zero immediately. Until it does, ovulation may be delayed or erratic. The first post-loss menstrual bleed can involve a thicker endometrial lining shedding, which often means more cramping than usual. Tracking this cycle is clinically useful: if hCG does not return to zero, it may indicate retained pregnancy tissue, which requires further management.
4. The grief of miscarriage can be disenfranchised — and that makes it harder to heal
Disenfranchised grief is a term coined by researcher Kenneth Doka to describe grief that society does not fully acknowledge or sanction. Miscarriage grief is one of its clearest examples. Because the loss occurs before a certain visible threshold — no funeral, often no formal announcement, sometimes before others even knew about the pregnancy — women are frequently expected to recover quickly and silently.
Clinical psychology research, including a large-scale study published in the journal Psychological Medicine, has found that anxiety and depression following miscarriage can persist for over a year in a significant proportion of women, and that post-traumatic stress disorder symptoms are present in a meaningful subset. These are not signs of weakness or of being “too attached too soon.” They are normal responses to genuine bereavement, and they deserve to be treated as such.
5. Thyroid dysfunction is a frequently missed contributor to pregnancy loss
The thyroid gland — a small, butterfly-shaped organ in the neck — produces hormones that regulate almost every metabolic process in the body, including the hormonal environment necessary to sustain early pregnancy. Even mildly elevated thyroid-stimulating hormone (TSH) levels, still within a “normal” reference range, have been associated with increased miscarriage risk in some studies.
The nuance here is important: what counts as “normal” TSH for the general population may not be optimal for pregnancy. Many reproductive specialists aim for a TSH below 2.5 mIU/L in women trying to conceive or in early pregnancy, compared to the broader “normal” upper limit of around 4.0 to 5.0 mIU/L used in routine testing. Additionally, the presence of thyroid antibodies — even with normal TSH — is an independent risk factor for miscarriage that is not always screened for during standard workups.
If you have never had a full thyroid panel including TPO antibodies in the context of pregnancy loss, it is worth discussing with your doctor.
6. Polycystic ovary syndrome increases miscarriage risk through more than one mechanism
Polycystic ovary syndrome (PCOS) — a hormonal condition affecting ovulation and androgen levels — is often discussed primarily as a fertility challenge. What receives far less attention is the evidence that women with PCOS who do conceive face a moderately elevated risk of miscarriage compared to women without the condition.
The mechanisms are multiple. Insulin resistance — present in many women with PCOS — may impair endometrial receptivity and early placental development. Elevated luteinising hormone (LH) at the time of conception has been associated with poorer embryo quality in some research. Chronic low-grade inflammation, another feature of PCOS, creates a suboptimal uterine environment. The encouraging news is that these mechanisms are largely modifiable, and working with a reproductive endocrinologist to optimise metabolic and hormonal markers before and during pregnancy may meaningfully reduce risk.
7. Antiphospholipid syndrome is treatable — and is more common than many women know
Antiphospholipid syndrome (APS) is an autoimmune condition in which the immune system produces antibodies that attack phospholipids — fats found in cell membranes — causing blood clotting abnormalities and increasing miscarriage risk. It is one of the most important and treatable causes of recurrent pregnancy loss.
Despite this, many women are not tested for APS until they have experienced multiple losses. The condition is diagnosed via blood tests — specifically for anticardiolipin antibodies, beta-2 glycoprotein I antibodies, and lupus anticoagulant — performed on two separate occasions at least 12 weeks apart. Women with confirmed APS can be treated with low-dose aspirin and low molecular weight heparin during pregnancy, a protocol supported by strong clinical evidence and associated with significantly improved live birth rates.
8. Your partner’s grief is real, and it may look nothing like yours
The emotional experience of miscarriage is not limited to the person who was pregnant. Partners — regardless of gender — frequently experience profound grief following pregnancy loss. What is less acknowledged is that their grief often manifests differently: more quietly, more inwardly, sometimes more rapidly suppressed under the pressure to “be strong.”
Research on partners’ experiences of miscarriage consistently shows elevated rates of anxiety and depression, with feelings of helplessness particularly prominent. Couples sometimes find that their grief timelines diverge sharply: one person is still acutely grieving weeks or months later while the other has moved into a functional coping mode, creating distance and misunderstanding. Couples therapy with a practitioner experienced in perinatal loss can be a genuinely useful tool — not because the relationship is in crisis, but because grief of this kind benefits from a structured space.
9. Miscarriage does not cause infertility — but the fear of it can alter your next pregnancy experience profoundly
One of the most pervasive myths surrounding miscarriage is that it damages fertility or reduces the chance of a successful future pregnancy. For the vast majority of women, this is not true. After a single miscarriage, the probability of a subsequent successful pregnancy is not meaningfully reduced. After two losses, the live birth rate in the following pregnancy remains encouraging. Even after recurrent miscarriage, specialist-supported pregnancies often result in successful outcomes.
What miscarriage can alter — and what is rarely addressed in clinical settings — is the psychological experience of a subsequent pregnancy. Post-loss pregnancies are frequently characterised by heightened anxiety, hypervigilance, and difficulty bonding or “allowing” hope until a certain milestone is passed. This is sometimes called pregnancy after loss anxiety, and it is a recognised psychological phenomenon that benefits from active support rather than simple reassurance. (For more on managing anxiety in pregnancy, see our guide to emotional wellbeing in the first trimester on webzalo.com.)
10. “Just try again” is not a treatment plan
The response many women receive following a first or even second miscarriage is some version of encouragement to try again without investigation. While this is statistically reasonable — the majority of first miscarriages are chromosomal events unlikely to recur — it does not account for women with underlying conditions that will cause loss to recur unless identified.
It also entirely dismisses the woman in front of the clinician: her grief, her need for understanding, her body’s signals. Even when no medical investigation is indicated, a post-loss consultation should involve space for the woman’s experience, basic guidance on emotional recovery, and clarity about when to escalate concerns. “Just try again” delivered without context or compassion is not merely insensitive — it is, in many cases, incomplete care.
Comparison Table: Common Investigations After Miscarriage
| Investigation | What It Tests | When Recommended | Specialist |
|---|---|---|---|
| Full thyroid panel (TSH + T4 + TPO antibodies) | Thyroid function and autoimmunity | After any miscarriage, especially if 2+ | GP or endocrinologist |
| Antiphospholipid antibody screen | Blood clotting autoimmunity (APS) | After 2+ miscarriages, or with fetal loss | Gynaecologist / haematologist |
| Karyotyping (parental) | Chromosomal translocations in parents | After 2–3 miscarriages | Clinical geneticist |
| Hysteroscopy or saline sonography | Uterine anatomy (fibroids, septum, polyps) | After 2+ miscarriages | Reproductive gynaecologist |
| Progesterone level (mid-luteal) | Luteal phase adequacy | After 2+ miscarriages, irregular cycles | Gynaecologist / endocrinologist |
| PCOS hormone panel (LH, FSH, AMH, insulin) | Metabolic and ovulatory function | After miscarriage with irregular cycles | Reproductive endocrinologist |
| Uterine natural killer cell biopsy | Immune environment of endometrium | Recurrent unexplained miscarriage | Reproductive immunologist |
The 3 Hopeful Facts That Can Change Everything
Hopeful Fact 1: The Live Birth Rate After Recurrent Miscarriage Is Higher Than Most Women Are Told
Clinical consensus — supported by data from multiple large-scale cohort studies — is that even after three consecutive miscarriages, the majority of women who receive specialist evaluation and appropriate treatment go on to have at least one successful live birth. In studies examining couples with unexplained recurrent miscarriage who received supportive care (regular early pregnancy monitoring, empathetic clinical management), live birth rates in subsequent pregnancies of 65 to 75 per cent have been reported. When an underlying cause is identified and treated — such as APS, thyroid dysfunction, or a uterine septum — outcomes improve further.
This is not a statistical platitude. It is a clinical reality that should be communicated to every woman who walks into a recurrent miscarriage clinic.
Hopeful Fact 2: Progesterone Supplementation in Early Pregnancy Is Showing Real Promise
For many years, the use of progesterone supplementation in early pregnancy was contested — prescribed variably with limited consensus. The landscape has changed. A large, well-designed clinical trial, the PRISM trial, found that vaginal progesterone supplementation in women with early pregnancy bleeding and a history of miscarriage significantly increased live birth rates compared to placebo in that subgroup.
Progesterone — the “pregnancy-sustaining” hormone — supports the thickening and maintenance of the uterine lining and modulates immune responses that could otherwise trigger pregnancy loss. While it is not a universal intervention, it is now a clinically supported option for specific women, and the evidence base continues to strengthen. If you have experienced miscarriage and find yourself bleeding in early pregnancy, it is worth asking your gynaecologist specifically about progesterone supplementation and whether you are a candidate.
(For more on hormonal support in early pregnancy, explore our article on progesterone and the first trimester on webzalo.com.)
Hopeful Fact 3: Specialist Miscarriage Care Genuinely Changes Outcomes
The existence of dedicated recurrent miscarriage clinics — staffed by reproductive gynaecologists, reproductive immunologists, and, in the best settings, perinatal psychologists — represents one of the clearest improvements in women’s reproductive healthcare in the past two decades. Research comparing outcomes in women seen in dedicated miscarriage units versus general gynaecology outpatient settings consistently shows better investigation rates, earlier identification of treatable causes, and, critically, higher live birth rates.
This matters because it affirms something essential: attentive, specific, patient-centred care works. You are not obligated to accept “this just happens sometimes” as your final answer. Asking for a referral to a specialist miscarriage service is an entirely reasonable next step after two or more losses — and in some clinical settings, after one loss if you have other risk factors or are over 35.
In My 19 Years of Clinical Practice…
In my 19 years of clinical practice, what I’ve seen most often is the damage done by delay — not delay in treatment, necessarily, but delay in taking a woman’s experience seriously. A patient arrives in my office having had two miscarriages, having been told each time to wait, to try again, to be patient. What she has actually been doing is carrying a private weight of grief, fear, and self-blame that has been building unopposed for months or years, with no investigation, no explanation, and no roadmap. What strikes me consistently is not how fragile these women are, but how resilient they are despite having received so little. When I run a full panel — thyroid, antiphospholipid antibodies, progesterone, uterine anatomy — I find actionable findings in a meaningful proportion of women who were previously told their losses were simply bad luck. The biology is not always simple, and grief is never simple, but the gap between what is possible and what most women receive is still, in 2025, wider than it should be. You deserve both the investigation and the conversation.
When to See a Specialist: Specific Red Flags and Timelines
You should request a referral to a reproductive gynaecologist or dedicated miscarriage clinic if any of the following apply:
Two or more consecutive miscarriages, regardless of your age. The three-loss threshold before investigation is increasingly regarded as outdated by specialist opinion.
Any miscarriage after 10 weeks, particularly a missed miscarriage (where the embryo stopped developing but the body did not expel it spontaneously). Late first-trimester or second-trimester losses have distinct causes that warrant different investigation.
Unusually heavy or prolonged bleeding after a miscarriage — specifically, soaking more than two sanitary pads per hour for more than two hours, which may indicate retained tissue or, rarely, a coagulation disorder. Attend your emergency gynaecology unit the same day.
Signs of infection following a miscarriage: fever above 38°C, offensive vaginal discharge, severe abdominal pain, or a persistent feeling of being unwell beyond 48 hours. This requires same-day assessment.
Persistent positive pregnancy test three to four weeks after a confirmed miscarriage — see your GP promptly for repeat hCG testing to rule out retained tissue or, rarely, ectopic pregnancy.
Significant anxiety or depression affecting daily function at any point following a miscarriage — your GP can refer you to a perinatal mental health service or a therapist experienced in pregnancy loss. This is a clinical referral, not a supplementary one.
You do not need to have reached a specific number of losses before advocating for yourself. Asking for investigation is not catastrophising. It is good clinical care — and you are entitled to it. (See also our webzalo.com guide to navigating gynaecological appointments and getting the referrals you need.)
You Have Not Failed. You Are Not Alone. Here Is Your Next Step.
Pregnancy loss carries a particular cruelty in how invisible it often is — to colleagues, to extended family, sometimes even to the healthcare system. But what I want you to take away from everything you have read here is this: most causes of recurrent miscarriage are either treatable or provide meaningful understanding. You are not simply unlucky. You are not too old. You are not being punished. And you are not at the end of any road.
The single most important thing you can do right now is book an appointment — with your GP, with a gynaecologist, or directly with a recurrent miscarriage service if your healthcare system allows self-referral — and bring this question: “What investigations are available to me, and when should we begin them?”
That is your next step. Not a Google spiral at 2am. Not silence. A conversation, with a clinician who can actually run tests, interpret results, and build a plan with you. You deserve that conversation. Now go and ask for it.
This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before making any changes to your health or treatment plan.