You Googled This at 2am. Here Is What You Actually Need to Know.
You noticed something. Maybe it was a small amount of blood on the tissue paper that made your heart drop into your stomach. Maybe it was a cramping sensation low in your pelvis that felt different from the gentle tugs and pulls of early pregnancy. Maybe your breasts, which had been tender since the day your test turned positive, suddenly felt completely normal, and that absence felt wrong in a way you could not explain.
So you picked up your phone, typed something into the search bar, and now you are here.
First: you are not overreacting. Your instinct to pay attention to your body during pregnancy is not anxiety. It is information-seeking, and it is entirely rational.
What you are looking for right now is clarity. Not panic, not false reassurance. You want someone to tell you, plainly and honestly, what these signs might mean, which ones require immediate action, and which ones can wait until your next scheduled appointment.
That is exactly what this article will give you.
These seven signs of miscarriage are presented not to frighten you, but because knowledge, delivered calmly and accurately, is always better than uncertainty. Understanding what your body is communicating gives you the ability to act at the right moment, for the right reasons.
What a Miscarriage Actually Is: The Clinical Foundation
A miscarriage, known medically as a spontaneous abortion, is the loss of a pregnancy before 24 weeks of gestation. The vast majority of miscarriages occur in the first trimester, defined as the first 12 weeks of pregnancy.
Think of early pregnancy like a complex, precisely timed biological negotiation. The embryo must implant successfully in the uterine lining, produce the right hormones to signal its presence to your body, and develop according to a very precise genetic blueprint. When something interrupts any stage of that process, whether chromosomal, hormonal, structural, or immunological, the pregnancy may not continue. This is not a failure of your body. It is often your body recognising, at the cellular level, that the conditions for a viable pregnancy are not in place.
This is one of the most critically misunderstood aspects of early pregnancy loss.
Featured Snippet Target: The signs of miscarriage include vaginal bleeding, pelvic cramping, the passage of tissue or fluid, and a sudden loss of pregnancy symptoms. Not all bleeding in early pregnancy means miscarriage, but any combination of these symptoms, particularly heavy bleeding with cramping, warrants prompt medical evaluation. Early assessment allows clinicians to determine the type of pregnancy loss and guide appropriate care.
Research suggests that somewhere between 10% and 20% of known pregnancies end in miscarriage, with the actual figure likely higher when accounting for very early losses before a positive test is even taken. Despite how common it is, miscarriage remains deeply underserved in mainstream medical education and public health communication. Women are often given very little clinical information about what to expect, what to watch for, and when a symptom crosses from “normal early pregnancy variation” into “please go to your nearest emergency department.”
That gap is what this article addresses directly.
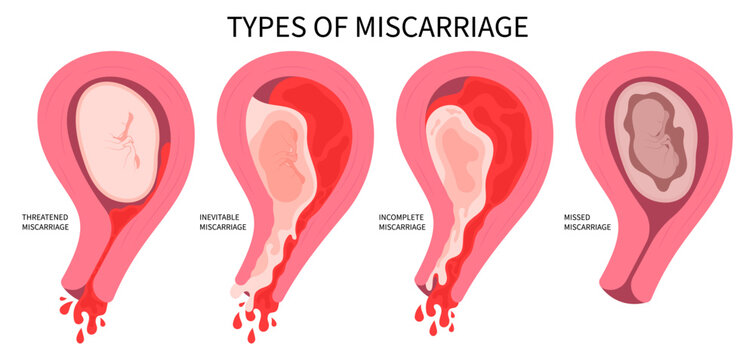
One important distinction to understand before we go further: a threatened miscarriage (where bleeding occurs but the cervix remains closed and the pregnancy may still be viable) is clinically different from an inevitable, incomplete, or complete miscarriage. Knowing the signs of miscarriage does not mean your pregnancy is lost. It means you have the information to seek the right care, at the right time.
7 Signs of Miscarriage You Need to Recognise
FORMAT A: Signs and Symptoms
1. Vaginal Bleeding That Is More Than Light Spotting
Bleeding in early pregnancy is one of the most common reasons women attend early pregnancy units, and not all of it signals miscarriage. Implantation bleeding, for example, can occur around the time of your expected period and is typically very light, lasting one to two days, and brown or pink in colour rather than red.
The bleeding that warrants immediate clinical evaluation is different. Heavy red bleeding that requires you to change a pad, bleeding that is accompanied by passing clots, or bright red bleeding that persists beyond a day are all signs that need urgent assessment.
Here is the clinical nuance that many women are not told: the volume and colour of the bleeding do not always correlate with the outcome. Some women bleed heavily and go on to have entirely healthy pregnancies. Others experience what looks like light spotting and are miscarrying. This is precisely why bleeding in pregnancy, particularly in the first trimester, should always be assessed rather than waited out. The only way to know what is happening is through an ultrasound and hormone testing.
If you experience any red vaginal bleeding in early pregnancy, contact your midwife, GP, or early pregnancy unit. You do not need to wait until it becomes heavy to seek advice.
miscarriage
2. Pelvic Cramping That Feels Distinct From Normal Pregnancy Discomfort
Mild pelvic cramping in early pregnancy is entirely normal. The uterus is growing, the ligaments supporting it are stretching, and implantation itself can cause a brief, cramping sensation. Many women describe normal early pregnancy as feeling similar to mild premenstrual tension in the lower abdomen.
The cramping associated with miscarriage is different in character and intensity.
It tends to be rhythmic, wave-like, and noticeably stronger than typical early pregnancy discomfort. Some women describe it as similar to strong period pain or labour-like contractions, occurring in intervals rather than as a constant dull ache. When this type of cramping accompanies any bleeding, even light bleeding, it becomes a more significant clinical indicator. The combination of cramping and bleeding together is more clinically significant than either symptom in isolation, and this combination should prompt a same-day call to your healthcare provider or a visit to an early pregnancy unit.
Lower back pain that radiates into the pelvis alongside cramping is also worth noting, particularly if it feels more intense than your usual back discomfort.
3. The Passage of Tissue, Clots, or Fluid From the Vagina
This is the sign that many women are not adequately prepared for, and it is one that warrants very clear, frank information.
During a miscarriage, the body passes the pregnancy tissue, which can include clots, membrane-like material, or greyish-white tissue. This can happen at home, often in the bathroom, and it can be deeply distressing if you do not know what you are seeing or what to do.
If you pass anything from your vagina during pregnancy that looks like tissue, clots larger than a 50-pence coin, or any fluid that is not normal vaginal discharge, this requires immediate medical evaluation. In some cases, clinicians will ask you to retain the passed tissue in a clean container so it can be sent for laboratory analysis. This analysis, where possible, can help determine whether the miscarriage was chromosomally related, which is an important piece of information for any future pregnancy planning.
Do not be embarrassed or distressed about presenting to an emergency department with passed tissue. This is clinically valuable information, and healthcare teams are well-trained to handle this with sensitivity.
4. A Sudden, Complete Loss of Pregnancy Symptoms
This is one of the signs of miscarriage that women often describe as the first thing they noticed, and it is one of the least discussed.
Early pregnancy symptoms, including breast tenderness, nausea, fatigue, and heightened sense of smell, are driven primarily by rising levels of human chorionic gonadotropin (hCG), the hormone produced by the developing placenta. When a pregnancy is no longer viable, hCG levels begin to fall, and the symptoms tied to those hormone levels often diminish or disappear.
Some women describe waking up one morning and realising their breasts no longer hurt, their nausea had lifted overnight, and they simply felt “normal” again. That sudden cessation of symptoms, particularly when it happens abruptly rather than gradually, can be an early indicator of a missed miscarriage, a situation where the embryo has stopped developing but the pregnancy has not yet passed.
It is worth noting that many pregnancy symptoms naturally reduce around 10 to 14 weeks as the placenta takes over hormone production. The distinction lies in timing and abruptness. If your symptoms fade gradually after 10 weeks, this is often normal physiology. If they disappear suddenly and you are still in the first trimester, a check-in with your midwife or GP is entirely appropriate.
A single absent symptom is rarely cause for immediate concern. A sudden, complete loss of multiple symptoms together, especially before 10 weeks, is worth discussing with your healthcare provider promptly.
5. Unusual Vaginal Discharge or an Odour That Was Not Present Before
This is a sign that does not appear on most miscarriage symptom lists, yet it carries real clinical importance.
During any stage of pregnancy loss, particularly an incomplete miscarriage where not all of the pregnancy tissue has passed naturally, there is an increased risk of infection. Signs of infection in the context of pregnancy loss include a vaginal discharge that has changed in colour to yellow, green, or grey, a new or unusual odour, and fever or chills.
An infected miscarriage, known clinically as a septic miscarriage, is a medical emergency. Though it is not the most common complication of early pregnancy loss, it is one that can progress quickly and requires immediate hospital treatment, typically intravenous antibiotics.
If you have recently experienced or are currently experiencing symptoms that suggest a miscarriage, and you develop a temperature above 38 degrees Celsius, unusual discharge, or a general feeling of being unwell that is out of proportion to what you were feeling before, do not wait for a scheduled appointment. Go to your nearest emergency department.
The key clinical insight here is that the risk of infection does not only apply to women who have had a medically managed or surgical miscarriage. It can occur following a natural or expectant miscarriage as well, particularly if any tissue remains in the uterus.
6. Shoulder Tip Pain Combined With Abdominal Symptoms
This is the sign of miscarriage that very few people know about, and it is critically important.
Shoulder tip pain, a sharp or aching pain at the very top of the shoulder near where the shoulder meets the neck, is not a musculoskeletal symptom in this context. It is a red flag for internal bleeding.
When blood collects in the abdominal cavity, it rises and irritates the diaphragm, the large flat muscle that separates the chest from the abdomen. The phrenic nerve, which runs from the neck down to the diaphragm, refers that irritation upward as pain felt at the tip of the shoulder. This is called referred pain.
In the context of pregnancy, shoulder tip pain alongside abdominal pain, dizziness, or faintness is a potential indicator of an ectopic pregnancy that has ruptured, rather than a miscarriage in the traditional sense. An ectopic pregnancy is one that has implanted outside the uterus, most commonly in the fallopian tube. A ruptured ectopic pregnancy is a life-threatening medical emergency and requires immediate surgical intervention.
If you experience shoulder tip pain at any point in early pregnancy, alongside any other concerning symptoms, you must attend your nearest emergency department immediately. This is not a symptom that warrants a phone call to your GP first. It warrants going directly to A&E.
This symptom deserves its own prominent place on any list of signs of miscarriage, precisely because it is so rarely included, and because missing it has serious consequences.
7. Dizziness, Faintness, or a Racing Heartbeat During Early Pregnancy Symptoms
Mild dizziness in early pregnancy is common, usually caused by blood pressure changes and the increase in blood volume that begins almost immediately after conception. That ordinary dizziness tends to be positional, meaning it is worse when you stand quickly, and it resolves within seconds.
The dizziness and faintness associated with a complicated miscarriage or ectopic pregnancy is qualitatively different. It is more intense, may come on without a postural trigger, and is often accompanied by pallor, cold sweating, or a rapid heartbeat. These are symptoms of haemodynamic compromise, meaning your blood pressure is dropping in response to significant internal or external blood loss.
According to current guidance from the NHS on ectopic pregnancy and early pregnancy loss, women who experience significant dizziness, faintness, or collapse alongside vaginal bleeding in early pregnancy require emergency medical assessment without delay.
Heavy bleeding outside the uterus or within the uterine cavity can lead to a rapid drop in blood pressure. Your body responds by increasing heart rate to try to maintain circulation. If you feel faint, notice your heart is racing, or feel as though you might collapse, this is a medical emergency regardless of how much visible bleeding you can see.
Internal bleeding, particularly in cases of ectopic pregnancy, can be significant without producing proportionally heavy external bleeding. The absence of heavy external bleeding does not mean the situation is clinically stable.
A Deeper Look at Miscarriage Types: What You May Not Have Been Told
Understanding the different clinical classifications of miscarriage helps you make sense of what your healthcare team is assessing and why certain symptoms matter more in certain contexts.
Threatened Miscarriage
A threatened miscarriage is defined as bleeding in early pregnancy where the cervix remains closed and the pregnancy may still be viable. This is one of the most common presentations in early pregnancy units. Many threatened miscarriages do not progress to pregnancy loss. Management typically involves rest, repeat hCG blood tests to check whether hormone levels are rising as expected, and an early ultrasound.
Missed Miscarriage
A missed miscarriage, also called a silent miscarriage, occurs when the embryo stops developing but the pregnancy has not yet passed. There may be no heavy bleeding or significant cramping. The main indicator is often the sudden loss of pregnancy symptoms described in sign number four above, confirmed on ultrasound. This type of miscarriage is particularly difficult emotionally because the body has not yet responded to the loss, and many women describe feeling “stuck in the middle” while awaiting either natural passage or medical management.
Incomplete Miscarriage
An incomplete miscarriage occurs when some, but not all, of the pregnancy tissue passes naturally. Bleeding may be heavier and more prolonged than in a complete miscarriage, and there is an increased risk of infection if retained tissue is not addressed. Management options include expectant care (allowing the body to complete the process naturally), medical management using medication to help the uterus contract and expel the remaining tissue, or surgical management.
Complete Miscarriage
A complete miscarriage has occurred when all the pregnancy tissue has passed and the uterus is empty on ultrasound. Bleeding typically reduces significantly once this happens. Follow-up with your healthcare provider is still important to confirm the uterus is clear and to discuss emotional support and next steps.
Ectopic Pregnancy
While technically distinct from a uterine miscarriage, ectopic pregnancy shares several early warning signs and is a critical part of any conversation about early pregnancy loss. An ectopic pregnancy occurs when a fertilised egg implants outside the uterus. It cannot develop into a viable pregnancy and requires prompt treatment. Signs include one-sided pelvic pain, vaginal bleeding, shoulder tip pain, dizziness, and faintness.
Research published through the American College of Obstetricians and Gynecologists (ACOG) on ectopic pregnancy management confirms that ectopic pregnancy remains one of the leading causes of maternal mortality in the first trimester, making early recognition and treatment essential.
What Causes Miscarriage: Understanding the Root Causes
One of the most painful and persistent myths surrounding miscarriage is that something the woman did caused it. Exercising. Eating the wrong food. Being stressed. Lifting something. Having sex.
Let the record be clear on this: in the vast majority of cases, nothing you did caused your miscarriage.
The most common cause of first-trimester miscarriage is chromosomal abnormality in the embryo. This occurs during the very earliest stages of cell division and is entirely outside anyone’s control. Clinical estimates suggest that chromosomal issues account for approximately 50% to 70% of all first-trimester losses.
Other recognised causes include:
Hormonal Factors Insufficient progesterone levels in early pregnancy can compromise the uterine lining’s ability to support implantation and the developing embryo. Low progesterone in the luteal phase, the second half of the menstrual cycle, is a recognised contributing factor in recurrent miscarriage. This is an area where clinical management is possible and increasingly common.
Uterine Structural Abnormalities Septate uterus (where a fibrous tissue band divides the uterine cavity), fibroids (non-cancerous growths in the uterine wall), and other structural variations can interfere with implantation or foetal development. Many of these conditions are diagnosable and, in some cases, treatable.
Thyroid Dysfunction Both an underactive thyroid (hypothyroidism) and an overactive thyroid (hyperthyroidism) have been associated with an increased risk of miscarriage. Thyroid function is routinely checked in women experiencing recurrent pregnancy loss, though it is less commonly tested following a single miscarriage. If you have any thyroid symptoms, including unexplained fatigue, weight changes, hair thinning, or palpitations, this is worth raising with your GP.
Antiphospholipid Syndrome (APS) APS is an autoimmune condition in which the body produces antibodies that increase the tendency of blood to clot abnormally. In pregnancy, this can interfere with blood flow through the placenta and is a recognised cause of recurrent miscarriage. It is diagnosable through a blood test and, critically, it is treatable. Women with APS are typically managed with low-dose aspirin and low-molecular-weight heparin during pregnancy, with good outcomes.
Infection Certain infections, including rubella, cytomegalovirus, listeria, and toxoplasmosis, can increase the risk of miscarriage, particularly in the first trimester. This is one of the reasons that antenatal screening includes checks for infectious diseases, and why food safety guidance during pregnancy is clinically grounded rather than precautionary box-ticking.
Age-Related Factors Egg quality declines with age, and chromosomal errors during egg development become more common as women move through their thirties and forties. This does not mean miscarriage is inevitable, but it does mean the risk increases with age, which is a clinical reality worth acknowledging openly.
Lifestyle Factors Smoking, heavy alcohol consumption, and very high caffeine intake have all been associated with an increased risk of miscarriage in clinical research. These are modifiable risk factors, and addressing them is one of the practical things within your control.
Managing the Emotional Reality of Pregnancy Loss
No article on the signs of miscarriage would be complete without acknowledging what comes alongside the physical symptoms: the emotional weight of it.
Miscarriage is grief. It is the loss of a pregnancy, yes, but for many women it is also the loss of a future they had already begun to imagine. It is the name they had been quietly testing in their minds. The due date they had marked mentally. The announcement they had been holding off on making.
This grief is legitimate and does not require a certain number of weeks to validate it.
The emotional aftermath of miscarriage is widely variable. Some women feel a deep sadness that lifts gradually over weeks. Others experience prolonged grief, anxiety about future pregnancies, or symptoms consistent with post-traumatic stress. Research in reproductive psychology increasingly recognises that pregnancy loss, at any gestation, can have a significant psychological impact that is frequently underacknowledged in primary care.
If you are struggling emotionally after a miscarriage, please know that this is not weakness. It is a completely understandable response to a real loss. There are specialist organisations, counsellors trained in pregnancy loss, and support communities that understand what you are going through in a way that general wellbeing advice simply cannot replicate.
The Miscarriage Association offers helplines, peer support, and clinically informed resources for women navigating pregnancy loss in the UK. Speaking to your GP about a referral to a counsellor specialising in reproductive grief is a legitimate and valuable next step.
You do not have to manage this alone.
What to Do After a Miscarriage: Recovery and Next Steps
Physical recovery after a miscarriage varies depending on how far along the pregnancy was and how the loss occurred.
Bleeding: Most women experience some vaginal bleeding for one to two weeks after a miscarriage. This is normal and expected as the uterus clears. If bleeding is heavier than a normal period for more than one to two days, or if it increases rather than decreases after initially settling, contact your healthcare provider.
Pain: Mild cramping in the days immediately following a miscarriage is common. Over-the-counter pain relief such as paracetamol is generally recommended. Ibuprofen is sometimes used but should always be discussed with your pharmacist or GP in the context of any underlying health conditions.
Infection awareness: As outlined in sign number five above, remain alert to signs of infection, including fever, unusual discharge, or feeling unwell beyond what you would expect from the miscarriage itself. Septic miscarriage is uncommon but requires prompt treatment.
Next menstrual period: Most women experience their first period approximately four to six weeks after a miscarriage. Ovulation typically resumes before this, meaning pregnancy is theoretically possible before your first period returns. Whether to try again quickly or to wait is a personal decision, ideally discussed with your healthcare provider based on your individual circumstances and the nature of the loss.
Follow-up testing: After a single miscarriage, routine investigation is not typically offered by the NHS, as most miscarriages are due to chromosomal factors and the chance of a successful subsequent pregnancy is high. After two or more consecutive miscarriages, referral to a recurrent miscarriage clinic is standard practice. At this clinic, investigations typically include blood tests for antiphospholipid antibodies, thyroid function, and clotting factors, as well as a pelvic ultrasound to assess uterine anatomy.
Your next pregnancy: The grief of miscarriage often amplifies anxiety in any subsequent pregnancy. This is an entirely normal response, and many early pregnancy units offer additional early reassurance scans for women with a history of pregnancy loss. You do not need to suffer through the anxiety of a subsequent first trimester alone. Ask your GP or midwife about what additional support is available to you.
Nutrition and Physical Recovery After Miscarriage
The body’s physical recovery from miscarriage is often underestimated.
Blood loss during miscarriage, particularly in incomplete or heavy miscarriages, can lead to iron deficiency, which presents as fatigue, pallor, breathlessness, and difficulty concentrating. A full blood count is a straightforward and entirely appropriate test to request from your GP in the weeks following a miscarriage.
Prioritising iron-rich foods, including red meat, legumes, leafy green vegetables, and fortified cereals, alongside vitamin C to enhance iron absorption, supports haematological recovery. If your blood count reveals low haemoglobin, your GP may recommend an iron supplement.
Folic acid remains important if you plan to try to conceive again. Clinical consensus holds that folic acid supplementation, started ideally before conception, reduces the risk of neural tube defects in a subsequent pregnancy. Most women are advised to continue or restart folic acid supplementation at 400 micrograms daily as soon as they are considering trying to conceive again.
Rest during recovery is not optional. It is physiological necessity. Your body has been through a significant hormonal shift and, in many cases, a physically demanding process. Gentle activity is appropriate, but returning to intense exercise too quickly can prolong recovery. Listen to your body’s cues and give yourself the same compassion you would offer a friend.
In My 19 Years of Clinical Practice: The Pattern I See Most Often
In my 19 years of clinical practice, what I’ve seen most often is women who knew. They had felt something shift. A heaviness in the pelvis, a quiet but persistent unease, a symptom that felt different from the gentle pulls of early pregnancy. They had Googled at midnight, called NHS 111 from the car park at work, shown up at the early pregnancy unit with apologetic eyes and the words “I probably don’t need to be here.”
You do need to be there.
What I have come to understand, through thousands of consultations and follow-up appointments, is that the single greatest gap in how early pregnancy loss is managed in mainstream healthcare is not in the tests we offer or the treatments we provide. It is in the information we give women before anything goes wrong. Women arrive at an early pregnancy unit frightened and uncertain not because they are anxious by nature, but because nobody sat them down and said, clearly and plainly, “here is what to watch for, and here is exactly when to come in.”
That absence of information creates confusion during an already extremely difficult time. It also, as I’ve seen with many patients, creates a painful secondary burden: the guilt of wondering whether they should have come in sooner. As I consistently explain: when you are not given clear guidance, you cannot be expected to make the right call. That responsibility belongs to the medical system, not to you.
If you take one thing from this article, let it be this. Coming in too early is never the wrong decision. An early pregnancy unit exists precisely for this moment.
When to See a Specialist: Specific Red Flags and Timeframes
The following symptoms require immediate medical attention. Do not wait for your next scheduled appointment for any of these.
Shoulder tip pain combined with abdominal pain or dizziness: Go directly to A&E. This is a potential indicator of ectopic pregnancy with internal bleeding and should be treated as an emergency until proven otherwise. Timeframe: immediately, without delay.
Heavy vaginal bleeding that soaks a pad within one hour or less: Attend your nearest emergency department immediately. Heavy blood loss in early pregnancy requires urgent assessment to rule out significant haemorrhage and to determine the cause. Timeframe: do not wait.
Fever of 38 degrees Celsius or above alongside any pregnancy loss symptoms: This raises the possibility of septic miscarriage and requires emergency assessment. Attend A&E immediately. Timeframe: immediately.
Fainting, collapse, or a racing heartbeat alongside abdominal pain or bleeding: Call 999 or attend A&E immediately. These are symptoms of haemodynamic instability. Timeframe: immediately.
Continued heavy bleeding for more than two weeks following a confirmed miscarriage: Book an urgent appointment with your GP or contact your early pregnancy unit. This may indicate retained pregnancy tissue requiring medical or surgical management. Specialist: gynaecologist or early pregnancy unit.
Two or more consecutive miscarriages: Request a referral from your GP to a dedicated recurrent miscarriage clinic. You do not need to wait for a third loss before asking. Investigations include antiphospholipid antibody testing, thyroid function, clotting studies, and pelvic ultrasound. Specialist: reproductive endocrinologist or gynaecologist specialising in recurrent pregnancy loss.
Persistent one-sided pelvic pain without heavy bleeding in early pregnancy: Request same-day assessment at an early pregnancy unit or attend your GP urgently. One-sided pain can indicate ectopic pregnancy even in the absence of heavy bleeding. Specialist: gynaecologist. Timeframe: same day.
You Are Not Alone: A Closing Note From Dr. Naomi
Pregnancy loss is one of the most disorienting experiences a woman can navigate, partly because it so often happens quietly, in private spaces, without the support structures that surround more visible forms of loss.
But you now have something that too many women face this moment without: clear, honest clinical information about what your symptoms might mean, and the confidence to act on it.
If you are experiencing any of the seven signs of miscarriage described in this article, the most important single step you can take right now is to contact your early pregnancy unit, your midwife, or your GP today. Not tomorrow. Not after the weekend. Today.
You are not being dramatic. You are not wasting anyone’s time. You are doing exactly what every pregnant woman should be supported to do: seeking assessment when something feels wrong.
Share this article with anyone in your life who is pregnant, or who is supporting someone through early pregnancy. The information in it could make a meaningful difference to someone’s outcome, and to their experience of a moment that is already difficult enough.
If you want to read more on this topic, explore our related articles on early pregnancy symptoms, hormonal causes of recurrent miscarriage, and what to expect from your first trimester.
You are your own best advocate. Now you know exactly when and how to use that voice.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before making any changes to your health or treatment plan.