How to Powerfully Reverse Unexplained Infertility in 90 Days: 8 Medically Proven Strategies That Finally Get Results
You’ve done every test. The results come back normal. And yet, month after month, pregnancy doesn’t happen. If that sentence feels like it was written specifically about your life, keep reading.
Unexplained infertility is one of the most emotionally draining diagnoses a woman can receive, not because the news is catastrophically bad, but because there is no clear enemy to fight. No blocked tube to fix. No hormonal disorder to treat. Just a giant question mark sitting in the middle of your reproductive future. And frustratingly, that question mark is more common than most people realize.
According to research published in Human Reproduction Open, up to half of all couples who seek medical assistance for infertility end up with a diagnosis of unexplained infertility. That means normal ovulation, at least one open fallopian tube, and normal sperm analysis, yet conception still isn’t happening. The causes, as the name suggests, remain largely unknown.
But here is what the science also tells us: “unexplained” does not mean “untreatable.” There are evidence-based, medically sound strategies that reproductive endocrinologists are using every single day to help couples with this diagnosis finally conceive. Some involve assisted reproductive technologies. Others involve surprisingly powerful lifestyle changes. And most of them can start working in as little as 90 days.
This guide walks you through eight of the most impactful strategies, each grounded in current clinical evidence, so you can walk into your next fertility appointment armed with real information and real options.
1. Understand What “Unexplained Infertility” Actually Means for Your Treatment Strategy
Before diving into solutions, it helps to understand the landscape. Unexplained infertility is not a permanent verdict. It is a working diagnosis assigned when standard fertility testing, covering semen analysis, ovulation confirmation, hormonal panels, and tubal patency, comes back within normal ranges, yet pregnancy has not occurred after 12 months of regular unprotected intercourse (or 6 months if you are over 35).
What makes this diagnosis tricky is that “normal” on a standard panel does not mean “optimal.” It means your results fall within a broad statistical reference range. Subtle issues with egg quality, embryo implantation, sperm-egg interaction, uterine receptivity, or even immune function may exist beneath the surface of a clean lab report. These are not always detectable with basic screening tools, which is why ongoing research into unexplained infertility keeps uncovering new biological mechanisms that standard testing simply misses.
The good news is that couples with unexplained infertility still retain inherent chances of natural conception, and those chances can be meaningfully improved with targeted interventions. Starting with the least invasive strategies and progressing methodically is not only medically sensible but often how pregnancies finally happen.
2. Optimize Your Fertility Diet to Directly Combat Unexplained Infertility
Food is not a magic cure. But it is one of the most underestimated levers you can pull when dealing with unexplained infertility, and the research is catching up to what many reproductive specialists have suspected for years.
A growing body of evidence points to the Mediterranean diet as the single most fertility-supportive eating pattern for women trying to conceive. This dietary approach, rich in leafy vegetables, whole grains, healthy fats from olive oil and nuts, legumes, fish, and lean poultry, is associated with improved IVF outcomes, better hormonal balance, and reduced systemic inflammation, all of which create a more hospitable environment for conception.
Evidence suggests that adherence to dietary patterns like the Mediterranean and pro-fertility diets may increase the chances of getting pregnant and having a live birth, likely due to anti-inflammatory and antioxidant mechanisms, weight regulation, and hormonal balance. On the flip side, Western-style diets high in saturated fat, refined sugar, and processed foods are associated with systemic inflammation and metabolic dysfunction that can negatively impact fertility potential.
Here is what to focus on when restructuring your diet for fertility:
- Load up on antioxidants. Berries, spinach, walnuts, and sweet potatoes help combat oxidative stress, which is a known contributor to poor egg quality and implantation failure.
- Prioritize plant protein over animal protein. Research from the Nurses’ Health Study found that swapping some animal protein for plant protein was linked to a lower risk of ovulatory infertility.
- Add healthy fats. Omega-3 fatty acids from salmon, sardines, flaxseeds, and walnuts support prostaglandin synthesis and hormone production in the reproductive system.
- Choose low-glycemic carbohydrates. Keeping blood sugar stable protects insulin sensitivity, which has a direct downstream effect on ovarian function and ovulatory regularity.
- Cut trans fats entirely. Trans fatty acids have been repeatedly identified as harmful to reproductive function in women.
A practical starting point: aim to fill half your plate with colorful vegetables at every meal, swap your afternoon processed snack for a handful of mixed nuts and berries, and eat fatty fish at least twice a week. These are not dramatic changes, but over 90 days, they add up to a meaningfully different hormonal and cellular environment.
3. Use Targeted Supplements Backed by Evidence to Support Unexplained Infertility Treatment
Supplements are a crowded, confusing space. Walk into any pharmacy and you will find dozens of products claiming to “boost fertility,” most of which are marketed more aggressively than they are studied. However, a handful of nutrients do have credible scientific backing, and for women with unexplained infertility, getting these nutrients right can make a measurable difference.
Scientific evidence is clear that while there is no single supplement that can reverse infertility, certain supplements may be beneficial, including CoQ10, which may improve egg quality, enhance the ovarian response to fertility treatments, and increase fertilization and pregnancy rates, especially for women over 35 or those with diminished ovarian reserve.
Here are the supplements with the strongest evidence for women with unexplained infertility:
Coenzyme Q10 (CoQ10): This antioxidant plays a central role in mitochondrial energy production inside egg cells. Mitochondrial function declines with age, which is why egg quality tends to drop after 35. CoQ10 supplementation, typically in doses of 200 to 600 mg per day, has been shown to support ovarian response in multiple studies. It takes about 90 days of supplementation to see measurable effects on egg quality, which aligns perfectly with a structured 90-day fertility plan.
Vitamin D: Low serum vitamin D is associated with infertility in normal-weight women, and research suggests it plays a role in regulating the immune environment of the uterus. Many women with unexplained infertility are subtly vitamin D deficient without knowing it. Ask your doctor to test your 25-OH vitamin D level. If it falls below 30 ng/ml, supplementation is strongly recommended.
Folic Acid (or Methylfolate): This is non-negotiable for anyone trying to conceive. Folic acid supports DNA synthesis, protects against early pregnancy complications, and has been associated with improved IVF outcomes. If you carry the MTHFR gene variant (a surprisingly common genetic mutation), your body may have difficulty converting synthetic folic acid into its active form. In that case, methylfolate, the bioavailable version, is a better choice. Ask your doctor about testing for this variant.
Myo-Inositol: This naturally occurring compound improves insulin sensitivity and supports ovarian function. It is well-studied in women with PCOS but is increasingly used for unexplained infertility as well, particularly in cases where subtle insulin resistance may be contributing to poor egg quality.
Iron: Low levels of ferritin, a protein that stores iron in the body, are associated with unexplained infertility. If your ferritin has not been tested as part of your fertility workup, request it specifically.
A note of caution: More is not better when it comes to supplements. High doses of some vitamins can actually be harmful to fertility. Always discuss any supplement plan with your reproductive endocrinologist before starting.

4. Pursue Ovulation Induction with IUI as a First-Line Unexplained Infertility Treatment
Once lifestyle modifications are in place, the next logical step in treating unexplained infertility is medically assisted conception, starting with the least invasive option: ovulation induction combined with intrauterine insemination (IUI).
IUI involves placing washed, concentrated sperm directly into the uterine cavity at the time of ovulation, bypassing the cervical mucus barrier and shortening the distance sperm must travel to reach the egg. When combined with oral medications that stimulate the ovaries to produce one or two eggs, the strategy significantly improves the odds of conception compared to timed intercourse alone.
Using both oral medications and insemination can significantly improve pregnancy rates for unexplained infertility, from about 5% per cycle with timed intercourse alone to notably higher rates with the combined approach. Medications used for ovulation induction in this context typically include clomiphene citrate (Clomid) or letrozole (an aromatase inhibitor), both of which stimulate follicular development by modulating estrogen signaling in the pituitary gland.
Here is what to expect during an IUI cycle:
- Day 2 to 5 of your cycle: Begin oral ovulation stimulation medication.
- Day 10 to 12: Ultrasound monitoring to check follicle development.
- Trigger shot: An injection of hCG to trigger ovulation when the follicle reaches maturity.
- IUI procedure: Performed 24 to 36 hours after the trigger shot. It takes about 5 to 10 minutes and is generally no more uncomfortable than a Pap smear.
- Two-week wait: Progesterone support may be recommended to support the luteal phase.
Most reproductive specialists recommend trying three to four IUI cycles before considering escalation to IVF. If you are under 35 and have been diagnosed with unexplained infertility, IUI with ovarian stimulation is typically the appropriate starting point before moving to more invasive and expensive interventions.
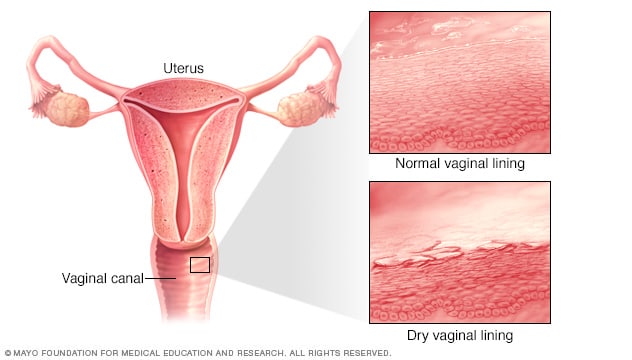
5. Investigate and Optimize Uterine Receptivity for Unexplained Infertility
Here is something that standard fertility testing often misses: the uterus itself may not be adequately “welcoming” to an embryo, even when all basic parameters appear normal. This is an area of active and exciting research in the field of unexplained infertility.
Groundbreaking research from the University of Melbourne, published in the Proceedings of the National Academy of Sciences (PNAS), identified that a molecule called miR-124-3p was elevated in the uterine lining of women with unexplained infertility. This molecule may contribute to making the endometrium inhospitable to embryo attachment, and targeted therapies to reduce it could help patients undergoing IVF achieve higher rates of success.
While that specific therapy is still in development, there are clinically available tests and interventions that can evaluate and improve uterine receptivity right now:
Endometrial Receptivity Analysis (ERA): A biopsy-based genetic test that identifies your personal “window of implantation,” the narrow time during your cycle when your uterus is most receptive to an embryo. Some women with unexplained infertility have a displaced implantation window, meaning embryo transfers done at the standard timing repeatedly fail. ERA can identify this and allow your doctor to time transfers more precisely.
Hysteroscopy: A minimally invasive procedure where a thin camera is passed through the cervix to directly visualize the inside of the uterus. It can detect and remove polyps, fibroids, adhesions, or subtle anatomical abnormalities that a basic transvaginal ultrasound or HSG might miss.
Uterine Natural Killer (uNK) Cell Testing: Elevated levels of certain immune cells in the uterine lining can prevent implantation. Some fertility specialists offer specialized immune testing and treatment, including low-dose steroids or intralipid infusions, for women with recurrent implantation failure or unexplained infertility.
If you have had multiple failed fertility treatments and everything appears structurally normal, pushing for a deeper uterine evaluation is a legitimate next step. It is the kind of investigation that can finally explain the unexplained.
6. Manage Stress Strategically, Because Chronic Stress Actively Undermines Unexplained Infertility Treatment
Let’s get one thing straight before we go further. Telling someone with unexplained infertility to “just relax and it will happen” is not only unhelpful, it is medically inaccurate. Stress alone does not cause infertility. However, chronic, unmanaged psychological stress does create a real physiological environment that can make conception harder.
High cortisol levels, the hallmark of chronic stress, disrupt the hypothalamic-pituitary-ovarian (HPO) axis, the hormone command chain that governs ovulation. Elevated cortisol can suppress gonadotropin-releasing hormone (GnRH), which is the signal that starts the entire ovulatory cascade. The result can be subtle cycle irregularities, luteal phase defects, or even anovulatory cycles, none of which would necessarily show up as “abnormal” on a standard fertility panel.
Chronic stress may interfere with ovulation and sperm production, and also increases cortisol levels, which can disrupt reproductive hormone balance. Yoga, journaling, breathwork, and even regular walks in nature can help reduce stress and regulate your body’s natural rhythm.
Here are evidence-informed stress management strategies worth incorporating into a 90-day fertility plan:
- Mind-body interventions: A study from Harvard Medical School found that women who participated in a structured mind-body program had significantly higher pregnancy rates than those who did not. Programs that combine relaxation techniques with cognitive behavioral therapy (CBT) are particularly effective.
- Acupuncture: Several small studies suggest acupuncture may improve IVF outcomes by supporting blood flow to the uterus and modulating stress hormone levels. The evidence is not definitive, but the risk is low and many women find it genuinely calming.
- Adequate sleep: Poor sleep directly elevates cortisol and disrupts the nocturnal hormone secretion patterns that are essential for reproductive function. Aim for 7 to 9 hours, with consistent sleep and wake times, as a non-negotiable part of your fertility protocol.
- Therapeutic support: Working with a psychologist or counselor who specializes in infertility can help you process the emotional weight of the diagnosis without letting it compound your biological challenges.
None of these strategies will work in isolation. But incorporated into a broader fertility plan, they create hormonal conditions that are noticeably more favorable for conception.
7. Achieve and Maintain a Fertility-Optimal Body Weight to Reverse Unexplained Infertility
Body weight has a more direct relationship with reproductive function than most women realize, and it operates in both directions. Both being underweight and being overweight can impair fertility, even in the absence of other identifiable diagnoses.
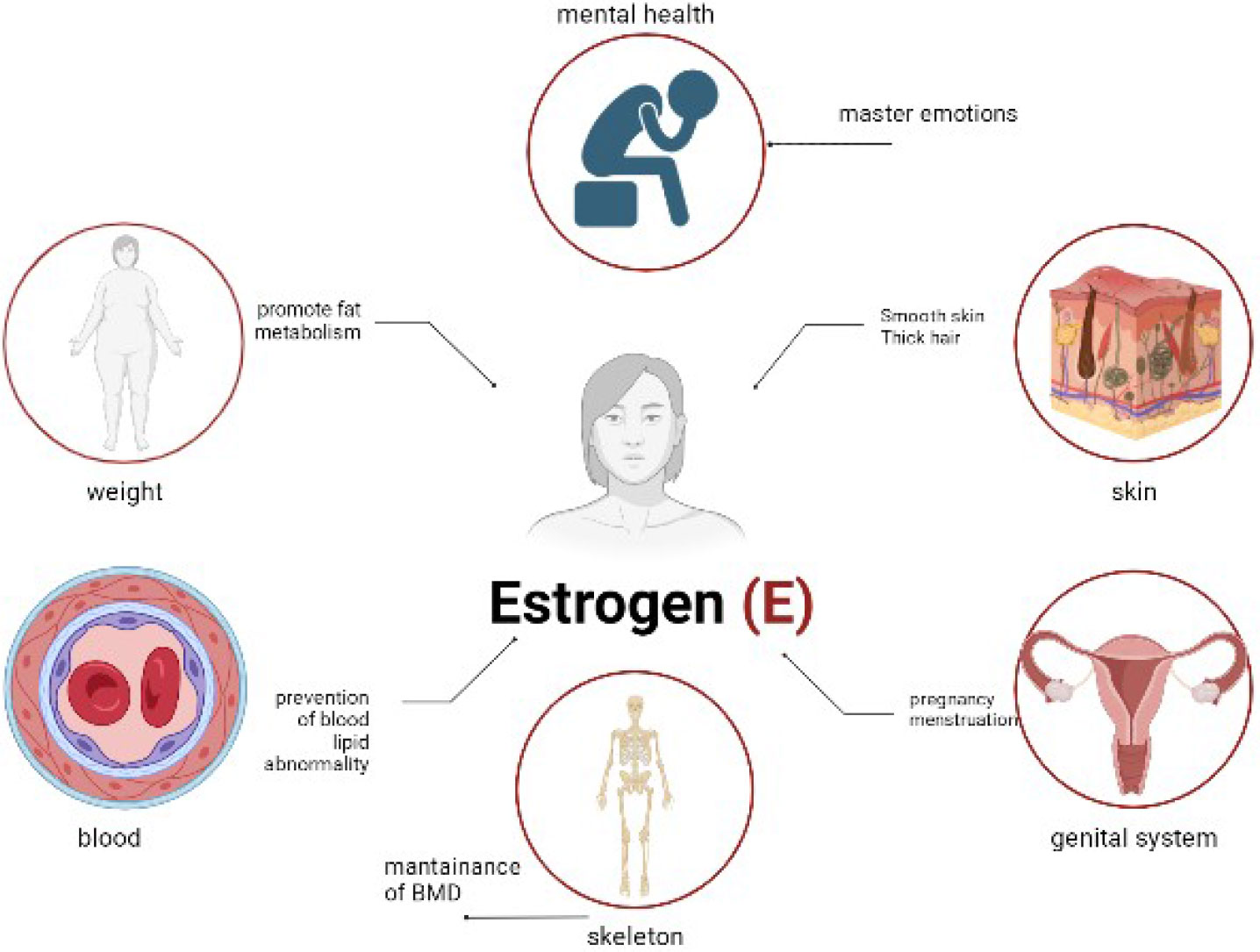
In women who are overweight or obese, excess adipose tissue produces estrogen independently of the ovaries, which can disrupt the normal hormonal feedback loops that govern ovulation. Insulin resistance, which commonly accompanies excess body weight, further compounds this effect by driving up androgen levels and interfering with follicle development. Meanwhile, underweight women may experience hypothalamic suppression of ovulation due to insufficient energy availability.
The sweet spot for fertility is a BMI between approximately 18.5 and 24.9, though it is worth noting that BMI is an imperfect metric and individual variation matters significantly. What matters most is not achieving a specific number but ensuring your body has adequate energy reserves to support both ovulation and early pregnancy.
For women with unexplained infertility who are in the overweight category, even a modest weight loss of 5 to 10 percent of body weight has been shown to restore regular ovulation and improve response to fertility medications. The approach matters too. Aggressive caloric restriction is counterproductive, as it increases cortisol, depletes key micronutrients, and can worsen hormonal imbalances. Sustainable, nutrient-dense eating, as described in the dietary strategy above, combined with regular moderate exercise, is the clinically recommended approach.
For women who are underweight or exercising excessively, the prescription is the opposite: reducing high-intensity exercise volume and ensuring adequate caloric and fat intake to support hormonal health. The ovary needs a stable energy signal from the body before it will release an egg reliably. When that signal is compromised by extreme dieting or overtraining, the reproductive system effectively goes quiet.
8. Consider In Vitro Fertilization (IVF) When First-Line Unexplained Infertility Treatments Fall Short
IVF is often spoken about as a last resort, but in the context of unexplained infertility, it is more accurately described as a diagnostic and therapeutic powerhouse. When a couple has not conceived after multiple IUI cycles and lifestyle optimization, IVF offers something no other treatment can: the ability to observe the fertilization process directly.
For many couples with unexplained infertility, IVF reveals what standard testing never could. Some couples discover that their eggs fertilize poorly in spite of normal sperm parameters, pointing to a subtle sperm-egg interaction problem. Others learn that their embryos develop poorly to the blastocyst stage, suggesting an underlying issue with embryo quality that timed intercourse could never overcome. Others still have excellent fertilization and blastocyst development, but fail to achieve implantation, which then opens the door to the uterine investigations described above.
According to the American Society for Reproductive Medicine’s guidelines on unexplained infertility, IVF is associated with the highest per-cycle live birth rates of all treatment options for unexplained infertility and is the appropriate next step when less invasive treatments have not succeeded.
Modern IVF for unexplained infertility often includes several additional tools:
Preimplantation Genetic Testing for Aneuploidies (PGT-A): Tests embryos for chromosomal abnormalities before transfer. This is particularly valuable for women over 35, where a significant proportion of eggs, and by extension embryos, carry chromosomal errors that prevent successful implantation or lead to early miscarriage.
Time-lapse embryo monitoring: Advanced incubator systems with built-in cameras allow embryologists to monitor embryo development continuously without disturbing the culture environment. This improves embryo selection and, in some clinics, is paired with AI-powered algorithms that predict which embryo is most likely to implant.
Intracytoplasmic Sperm Injection (ICSI): Rather than allowing sperm to fertilize eggs in a dish, ICSI involves injecting a single selected sperm directly into each egg. This is routinely used in unexplained infertility cases where conventional IVF has resulted in poor fertilization rates.
Frozen Embryo Transfers (FET): Freezing all embryos and transferring them in a subsequent, non-stimulated cycle can improve implantation rates by allowing the uterine environment to recover from the hormonal effects of stimulation before a transfer is attempted.
As with all fertility treatments, the success of IVF depends significantly on age, ovarian reserve, and clinic-specific factors. The World Health Organization’s 2025 guideline on infertility treatment recommends that IVF be offered when less invasive treatments have not achieved pregnancy, and that treatment decisions be individualized based on patient age, duration of infertility, and prognosis.
Comparison Table: Unexplained Infertility Treatment Strategies at a Glance
| Strategy | Type | Best For | Timeline to See Results | Invasiveness | Evidence Level |
|---|---|---|---|---|---|
| Fertility Diet (Mediterranean) | Lifestyle | All women trying to conceive | 3 to 6 months | None | Moderate to strong |
| Targeted Supplements (CoQ10, Vitamin D, Folic Acid) | Nutritional | Women over 35, low micronutrient levels | 90 days | None | Moderate |
| Stress Management & Sleep Optimization | Lifestyle | Women with high cortisol/cycle irregularities | 4 to 8 weeks | None | Moderate |
| Body Weight Optimization | Lifestyle | Women with BMI outside 18.5 to 24.9 range | 3 to 6 months | None | Strong |
| IUI with Ovulation Induction | Medical | First-line treatment, women under 38 | Per cycle (3 to 4 cycles recommended) | Minimal | Strong |
| Hysteroscopy / ERA Testing | Diagnostic | Recurrent implantation failure | Single procedure | Mild | Moderate |
| Uterine Immune Investigation | Diagnostic | Multiple failed IUI/IVF cycles | 4 to 8 weeks | Mild | Emerging |
| IVF with PGT-A / ICSI / FET | Medical | After failed IUI, women over 35, all unexplained cases | Per cycle (1 to 3 cycles typical) | Significant | Strongest |
A Realistic Picture: What “90 Days” Actually Looks Like
The 90-day framework used in this article is not arbitrary. It reflects two important biological realities. First, the human egg takes approximately 90 days to complete its final maturation process before ovulation, which means the dietary, supplement, and lifestyle changes you make today will directly influence the quality of the eggs you ovulate three months from now. Second, one complete IUI cycle, from stimulation to result, takes approximately four to six weeks, meaning three cycles fit neatly within a 90-day window.
This means that a well-structured 90-day plan could simultaneously involve starting the Mediterranean diet, addressing any identified micronutrient deficiencies, implementing consistent stress management practices, achieving weight stability if needed, and completing two to three IUI cycles, all while gathering the data needed to decide whether escalation to IVF is appropriate.
The key is to stop treating these strategies as either-or options and start treating them as a coordinated, layered protocol. Reproductive endocrinologists who specialize in unexplained infertility understand this approach well. If your current fertility provider is not discussing lifestyle optimization alongside medical treatment, that is a conversation worth initiating.
Conclusion
Unexplained infertility is one of the most disorienting diagnoses in reproductive medicine because the absence of a clear answer can feel like the absence of hope. But the evidence says otherwise. The strategies in this article represent a spectrum of real, clinically grounded approaches that are helping couples with this diagnosis conceive every day.
You do not have to do everything at once, and you do not have to do it alone. Start with the foundations: food, sleep, stress, and supplements. Layer in medical treatment at the appropriate level for your age, timeline, and clinical picture. Advocate for deeper investigations if standard approaches are not moving the needle. And find a reproductive specialist who treats you as a partner in the process, not just a patient waiting for a protocol.
The diagnosis is unexplained. Your determination does not have to be.
Take the Next Step
If this article helped you feel less alone and more informed, share it with a friend who is navigating the same journey. She deserves to know these options exist.
Drop a comment below: Have you been diagnosed with unexplained infertility? What has your experience been with any of these strategies? Your story might be exactly what another woman needs to hear today.
This article is written for informational purposes only and does not constitute medical advice. Always consult a qualified reproductive endocrinologist or healthcare provider before making changes to your fertility treatment plan.