7 Proven, Powerful Signs Your Fertility Is Declining After 30 (And Exactly What To Do Before It’s Too Late)
Your body has been sending you signals. You just didn’t know what they meant, until now.
If you’re a woman in your 30s and something feels “off,” whether it’s your period, your energy, your mood, or your ability to conceive, this post is written specifically for you. Because fertility decline after 30 is real, it is measurable, and most importantly, it is something you can actually do something about.
Introduction: The Thing Nobody Told You About Fertility After 30
Here is the uncomfortable truth that most women don’t hear until they are already sitting in a fertility clinic, feeling blindsided.
Fertility doesn’t fall off a cliff at 35. It starts declining gradually, quietly, and often without obvious drama well before that. The age of 30 is the biological inflection point where the pace of change begins to accelerate. Egg quantity begins to drop more noticeably. Egg quality starts to shift. Hormonal rhythms that have been humming along steadily for years begin to modulate.
And here’s what makes this particularly frustrating: most of the signs are subtle. They look like stress. They look like “getting older.” They look like a busy life catching up with you. So most women don’t connect the dots until they’ve been trying to conceive for six months or a year and suddenly find themselves in a doctor’s office wondering why nobody warned them.
This post is that warning. It is also the roadmap.
We’re going to walk through seven of the most powerful, clinically recognized signs that your fertility may be declining after 30. For each one, we’ll explain what it actually means biologically, why it matters, and exactly what steps you can take right now, whether you want to conceive soon, later, or you simply want to understand your body better.
Why Fertility Literacy Matters More Than Ever
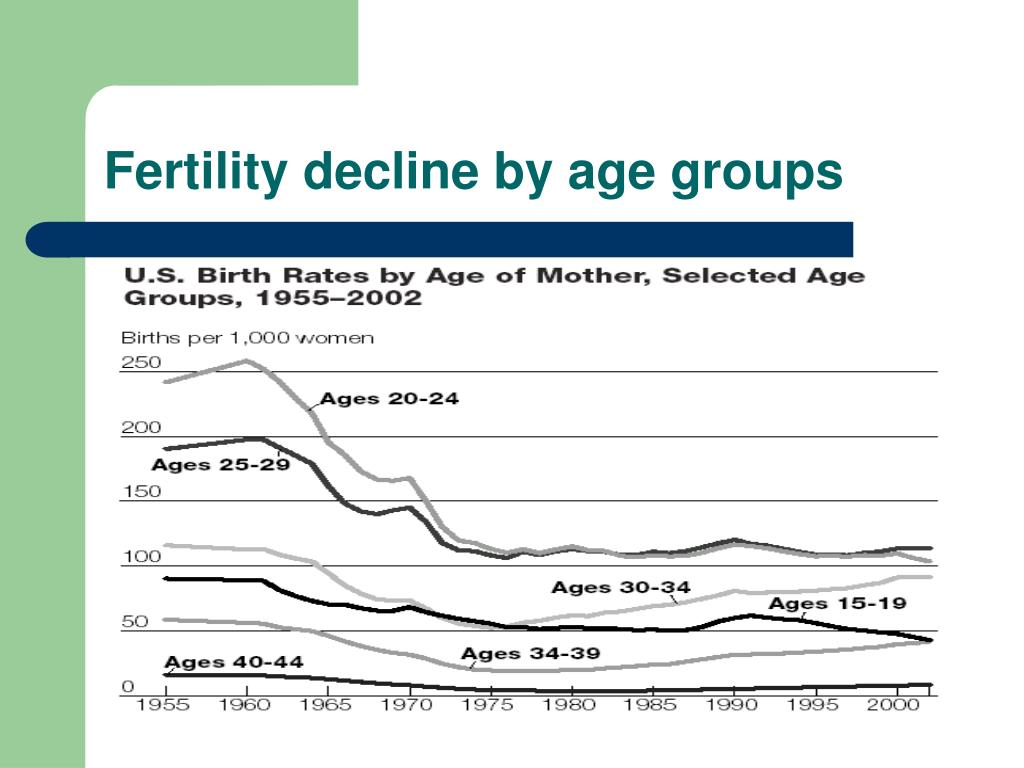
Women today are, on average, waiting longer to have children than any previous generation in recorded history. According to data from the U.S. Centers for Disease Control and Prevention, the average age of first-time mothers in the United States has risen from about 21 in 1972 to nearly 27 nationally, and considerably higher in urban and professional demographics. In major cities, first-time motherhood in the mid-to-late 30s is increasingly common.
None of this is inherently wrong. Women have careers, educational goals, financial considerations, relationship timelines, and personal readiness factors that are every bit as legitimate as the biological clock. The problem is not that women are waiting. The problem is that they are often waiting without accurate information about what their biology is doing in the meantime.
Reproductive medicine has made extraordinary advances. Egg freezing, IVF, preimplantation genetic testing, and a growing array of hormonal support protocols have expanded options meaningfully. But those options work best, are most successful, and are least emotionally and financially taxing when pursued with clear, timely information. The earlier you understand your fertility picture, the more tools you have at your disposal.
This is not a post about alarm. It is a post about information. And information, in this context, is one of the most powerful reproductive choices you can make.
Knowledge is not panic. Knowledge is power. Let’s get into it.
Sign #1: Your Periods Are Getting Shorter (A Major Fertility Decline After 30 Red Flag)
You’ve had a 5-day period your whole adult life. Lately, it’s wrapping up in 3. You’re secretly relieved. Less mess, less discomfort, done faster. But here’s the thing: a shortening menstrual cycle or a lighter, briefer period can be one of the earliest signs of declining ovarian reserve.
Here’s the biology in plain English. As you age, the number of eggs remaining in your ovaries (your “ovarian reserve”) decreases. With fewer follicles maturing each cycle, your body produces less estrogen in the first half of your cycle. Less estrogen means a thinner uterine lining. A thinner lining sheds faster and more lightly. What feels like a convenient change is actually your hormones quietly renegotiating the terms.
What a Shortening Cycle Actually Tells You
A cycle that used to be 28 to 30 days creeping down to 24 or 25 days is another related pattern worth noting. Shorter cycles often mean your follicular phase (the first half, where an egg matures) is compressing. That compression can reflect diminishing ovarian reserve and may reduce the window in which conception is possible each month.
This doesn’t mean you can’t get pregnant. It means the window may be narrowing, and the earlier you know that, the better your options.
What to do right now:
- Track your cycle carefully for 3 to 6 months using an app like Clue or Flo and note any changes in length, flow, and duration.
- Talk to your OB-GYN or a reproductive endocrinologist about an AMH (Anti-Müllerian Hormone) blood test, which measures ovarian reserve directly.
- Ask about a Day 3 FSH and estradiol test, which gives a snapshot of how hard your body is working to recruit eggs each cycle.
- Don’t dismiss lighter, shorter periods as a win without getting context. Your body is telling you something.
The earlier you detect a shift in your cycle, the earlier you can have an informed conversation about your options, including egg freezing, fertility preservation, or simply accelerating your timeline if having children is in your plans.
Sign #2: You’re Experiencing Irregular or Skipped Periods — A Classic Fertility After 30 Signal
Irregular periods are one of those things women tend to chalk up to stress, travel, a new workout routine, or just “one of those months.” And sometimes, that’s exactly what they are. But when irregularity becomes a pattern after 30, it deserves more attention than most women give it.
Ovulation is the cornerstone of fertility. No ovulation, no egg. No egg, no pregnancy. When your cycles become erratic, it often signals that ovulation itself is becoming irregular. This is sometimes referred to as oligovulation (infrequent ovulation) and it becomes increasingly common as ovarian reserve declines.
The Difference Between Occasional Irregularity and a Pattern
One wonky cycle after a transatlantic flight or a brutal work deadline is unlikely to be cause for alarm. But if you’re regularly skipping months, cycling every 21 days one month and every 38 the next, or going 60-plus days between periods with no obvious external trigger, those are patterns worth investigating.
Conditions like polycystic ovary syndrome (PCOS), thyroid dysfunction, and hyperprolactinemia can all cause irregular cycles and affect fertility. Perimenopause, which can begin as early as the mid-30s in some women, is another possibility. All of these are diagnosable and, importantly, manageable.
What to do right now:
- Log every cycle for at least three to six months, including start date, end date, flow level, and any notable symptoms like cramping or spotting.
- Request a hormone panel from your doctor that includes FSH, LH, AMH, estradiol, TSH (thyroid), and prolactin.
- If PCOS is suspected, ask about an ultrasound to assess antral follicle count (AFC), which is another measure of ovarian reserve.
- Consider seeing a reproductive endocrinologist (RE) rather than only a general OB-GYN if you’ve had irregularity for more than three consecutive cycles.
Irregular periods are your body waving a flag. The kindest thing you can do for your future self is to listen.
Sign #3: Changes in Cervical Mucus — An Underrated Sign of Declining Fertility After 30
This is the sign most women never learn about in school, in their doctor’s office, or from any conversation they’ve ever had. And it is, quietly, one of the most useful fertility indicators your body produces every single month.
Cervical mucus (CM) changes throughout your cycle in response to estrogen. In the days leading up to ovulation, it typically becomes clear, stretchy, and slippery, often compared to raw egg whites. This texture signals peak fertility and creates an environment that helps sperm survive and travel toward an egg. After ovulation, it thickens and dries up.
Why Less or No Fertile-Quality Mucus Matters
As estrogen production declines with age and reduced ovarian reserve, many women notice that their fertile-window mucus becomes less abundant, less stretchy, or disappears almost entirely. Some women in their mid-30s report that they used to have several days of egg-white cervical mucus in their 20s, and now they see almost none.
This matters because even if ovulation is still occurring, reduced CM can impair sperm mobility and reduce the chances of fertilization. It’s a fertility factor that rarely appears on a blood panel but has real-world conception implications.
What to do right now:
- Start observing and charting your cervical mucus daily. This costs nothing and takes seconds. Look for changes in texture, color, and consistency.
- Learn the Creighton Model or the Billings Ovulation Method, both of which are well-researched frameworks for understanding CM patterns.
- Ask your doctor about whether low-dose estrogen support or specific supplements (more on this shortly) might help.
- Stay well-hydrated. Dehydration can reduce CM quantity independently of hormonal factors.
- Avoid lubricants like K-Y Jelly during intercourse if trying to conceive, as many are spermicidal. Instead, look for fertility-friendly options like Pre-Seed.
Sign #4: Worsening PMS or New Mood Symptoms — A Hormonal Sign of Fertility Decline After 30
You’ve always been pretty even-keeled before your period. Maybe a little bloated, a little cranky, nothing you couldn’t handle. But lately? The week before your period feels genuinely hard. You’re irritable, anxious, tearful, or exhausted in ways that feel disproportionate to your circumstances. Your partner might have even gently, cautiously, asked if you’re okay.
What’s happening is hormonal, and it’s connected to fertility. As progesterone levels decline (which often occurs alongside declining ovarian reserve), the ratio between estrogen and progesterone can tip out of balance. This estrogen dominance in the luteal phase, the second half of your cycle, is a direct driver of worsening premenstrual symptoms.
The Progesterone Connection
Progesterone is often called the “calming hormone.” It has neurological effects, including supporting GABA activity in the brain, which promotes relaxation and emotional equilibrium. When progesterone drops, anxiety and mood instability often rise in lockstep. This is also the hormone that prepares and maintains the uterine lining for a potential pregnancy. Insufficient progesterone is a major cause of early miscarriage and implantation failure.
If your PMS has genuinely worsened after 30, especially if it’s accompanied by spotting before your period, that’s a signal that your luteal phase may be compromised.
What to do right now:
- Ask your doctor for a Day 21 progesterone test (or 7 days post-ovulation if your cycle is irregular). This measures whether you’re producing adequate progesterone after ovulation.
- Keep a detailed mood and symptom journal across your cycle. Apps like Moody or Clue allow you to log psychological symptoms alongside physical ones.
- Discuss luteal phase support with your doctor if progesterone is low. Options include natural progesterone supplementation (bioidentical), which is widely used in fertility treatment.
- Consider magnesium glycinate supplementation, which has solid research support for reducing PMS symptoms and supporting progesterone function.
- Reduce alcohol intake during your luteal phase. Alcohol impairs progesterone metabolism and can amplify hormonal imbalance.
Sign #5: Difficulty Conceiving After Three to Six Months of Trying — A Direct Fertility After 30 Indicator
This one may seem obvious, but it’s one that many women and couples underestimate in its clinical significance. The general medical guidance is that if you are under 35 and have been trying to conceive for 12 months without success, you should seek evaluation. But if you are 30 to 35, many reproductive specialists now recommend seeking evaluation after just six months of trying. And if you’re 35 or older, that window shortens to three months.
Why the age-based acceleration? Because time is genuinely a biological variable in fertility. The longer you wait to investigate, the fewer options may be available, and the more cycles you may spend in limbo without understanding why conception isn’t happening.
What “Trying” Actually Means
It’s worth defining terms. Medically, “trying to conceive” means having unprotected intercourse at least two to three times per week, including during the fertile window. If you’ve been having occasional unprotected sex without specifically timing it to ovulation, that’s a different picture than targeted, cycle-aware conception attempts.
Research from the American Society for Reproductive Medicine confirms that by age 30, a woman’s monthly fecundity rate (the probability of conceiving in any given cycle) has already begun to decline from the peak of approximately 25% in the mid-20s. By 35, it drops further still.
This is not meant to alarm you. It’s meant to calibrate your expectations and your timeline.
What to do right now:
- Use ovulation predictor kits (OPKs) to accurately identify your fertile window. Guessing based on cycle length alone can cause you to miss the window entirely.
- If you’ve been trying for six months or more without success, request a full fertility workup. This should include hormone panels, a semen analysis for your partner, and a hysterosalpingography (HSG) to check whether your fallopian tubes are open.
- Don’t wait for a full year if you have any of the other signs in this article. You can advocate for earlier testing.
- Consider getting a fertility consultation even before you’re actively trying if you’re in your early 30s and know you want children in the next few years.
Sign #6: Hot Flashes, Night Sweats, or Vaginal Dryness — Early Perimenopause Signs Linked to Fertility Decline After 30
When most people hear “hot flashes,” they picture women in their 50s fanning themselves at dinner parties. But perimenopause, the transitional period before menopause, can begin in a woman’s mid-to-late 30s, and occasionally even earlier. And the symptoms it produces are directly tied to declining estrogen and diminishing ovarian reserve.
Hot flashes are brief episodes of intense heat, often accompanied by sweating and a flushed face. Night sweats are their nocturnal equivalent. Vaginal dryness, reduced libido, and changes in skin and hair can also accompany this hormonal shift. These are not just comfort issues. They are fertility signals.
Early Perimenopause and What It Means for Your Fertility
Early perimenopause doesn’t mean you cannot conceive. Many women in early perimenopause do conceive, naturally and through assisted reproduction. But it does mean that your fertile window is contracting more rapidly than average, and that the conversations you might have planned to have “in a few years” may need to happen now.
The presence of vasomotor symptoms (the clinical term for hot flashes and night sweats) before the age of 40 is sometimes referred to as premature ovarian insufficiency (POI) when accompanied by diagnostic criteria, or as early perimenopause when it’s part of a natural but accelerated decline. Either way, it warrants medical attention and fertility-specific conversation.
What to do right now:
- Don’t dismiss hot flashes or night sweats as stress or anxiety if you’re experiencing them regularly before age 40. See a doctor.
- Ask for an FSH blood test drawn on Day 2 or Day 3 of your cycle. Elevated FSH is one of the clearest hormonal markers of diminishing ovarian reserve and early perimenopause.
- Request an AMH test, which does not need to be drawn on a specific cycle day and gives a good picture of remaining egg reserve.
- Discuss hormone therapy or fertility preservation options if POI or early perimenopause is confirmed.
- Address vaginal dryness proactively if you’re trying to conceive. Vaginal dryness can make intercourse uncomfortable, which affects frequency of attempts, and certain internal dryness can affect the environment sperm travel through.
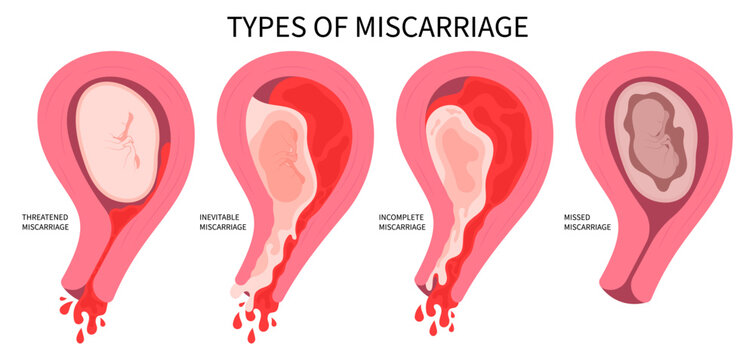
Sign #7: Recurrent Early Miscarriage — One of the Most Painful Signs of Fertility Decline After 30
This is the hardest sign to write about, and the hardest one to experience. If you have had one or more pregnancy losses, especially in the early weeks before 10 weeks, this section is written with full awareness of how painful that experience is.
Recurrent miscarriage (defined clinically as two or more pregnancy losses) affects approximately 1 to 2% of women overall, but the rate rises significantly with age. Most early miscarriages are caused by chromosomal abnormalities in the embryo, specifically aneuploidy, where the embryo has the wrong number of chromosomes and cannot develop to term. As egg quality declines with age, the rate of chromosomal errors in eggs increases. This is the primary biological reason why miscarriage rates rise after 30 and more sharply after 35.
This Is About Egg Quality, Not Just Quantity
The decline in fertility after 30 is not just about running out of eggs. It’s about the quality of the eggs that remain. A 32-year-old woman may have a perfectly adequate quantity of eggs but a growing proportion of those eggs may carry chromosomal errors that make them non-viable. This is why “you still have plenty of eggs” is not the whole story.
Recurrent early loss is your body’s signal that either egg quality, embryo quality, or uterine environment needs investigation. All three are workable problems with medical support.
What to do right now:
- After two or more losses, request a recurrent pregnancy loss (RPL) workup. This should include chromosomal testing of both partners, a uterine cavity evaluation (via sonohysterogram or hysteroscopy), thrombophilia screening, and a full hormone panel.
- Ask your fertility specialist about preimplantation genetic testing (PGT-A) if you’re considering IVF. This allows embryos to be screened for chromosomal normalcy before transfer, significantly reducing miscarriage risk.
- Discuss coenzyme Q10 (CoQ10) with your doctor. There is growing evidence that CoQ10 supplementation supports mitochondrial function in eggs, potentially improving egg quality. Doses used in research typically range from 400 to 600mg daily.
- Ensure your folic acid or methylfolate intake is adequate. Women with the MTHFR gene variant process folic acid less efficiently, and methylfolate is a better-absorbed alternative.
- Seek emotional support. Pregnancy loss is grief. It is valid, it is real, and processing it with a counselor or support group is not weakness. It is care.
The Fertility Decline After 30: What the Data Actually Shows
Here is a clear, honest snapshot of how age intersects with fertility metrics, based on available reproductive medicine data.
| Age Range | Monthly Chance of Conception | Miscarriage Rate | Egg Quality Decline | Recommended Action Timeline |
|---|---|---|---|---|
| 25 to 29 | ~25% per cycle | ~10 to 12% | Minimal | Baseline fertility awareness |
| 30 to 32 | ~20% per cycle | ~12 to 15% | Mild, gradual | Begin tracking; consider AMH test |
| 33 to 35 | ~15 to 18% per cycle | ~15 to 20% | Moderate | Seek evaluation after 6 months trying |
| 36 to 38 | ~10 to 12% per cycle | ~20 to 25% | Significant | Seek evaluation after 3 months trying |
| 39 to 40 | ~8 to 10% per cycle | ~25 to 35% | Considerable | Immediate fertility consultation |
| 40 to 42 | ~5 to 8% per cycle | ~35 to 50% | Substantial | Immediate consultation; discuss all options |
Sources: American Society for Reproductive Medicine; Society for Assisted Reproductive Technology (SART)
This table is not meant to induce panic. It’s meant to replace vague anxiety with clear information. A 15% monthly chance of conception is still meaningful. A 20% miscarriage rate means 80% of pregnancies don’t miscarry. The numbers create context, not certainty.
What You Can Actually Do: A Practical Fertility-Support Framework
Now that you know the signs, let’s talk about action. Because every single sign discussed above has a corresponding response, and most of them are things you can start today.
1. Get the Right Tests Done
The foundation of any fertility strategy is accurate information. The core tests you should request if you have any of the signs above include:
- AMH (Anti-Müllerian Hormone): Measures ovarian reserve. Can be done any day of your cycle.
- Day 3 FSH and Estradiol: Measures how hard your body is working to stimulate egg development. Done on cycle Day 2 to 4.
- Antral Follicle Count (AFC): An ultrasound-based count of resting follicles. Done in the first few days of your cycle.
- Day 21 Progesterone: Confirms that ovulation occurred and measures luteal phase adequacy.
- Thyroid Panel (TSH, Free T3, Free T4): Thyroid dysfunction is a major and frequently missed cause of fertility problems.
- Full hormonal panel: Including prolactin, LH, DHEA-S, and testosterone.
Many of these tests can be ordered by a general practitioner, but a reproductive endocrinologist will interpret them in the most fertility-relevant context.
2. Optimize What You Can Control
Not everything about fertility is fixed. Many lifestyle and nutritional factors have solid evidence behind them:
- CoQ10 supplementation (400 to 600mg daily): Supports mitochondrial energy in eggs and may improve egg quality, particularly relevant for women over 35.
- DHEA supplementation (25 to 75mg daily, under medical supervision): Some research supports DHEA for women with diminished ovarian reserve. This should only be taken under medical guidance as it is hormonally active.
- Mediterranean-style diet: Rich in leafy greens, legumes, healthy fats, and lean protein, with reduced processed foods and sugar. Consistently associated with better fertility outcomes in research.
- Reduce alcohol significantly: Even moderate alcohol consumption has been shown to reduce fertility and increase miscarriage risk.
- Manage thyroid health: Ensure your TSH is below 2.5 if you are trying to conceive. Many doctors consider values up to 4.5 “normal” for the general population but reproductive medicine specialists generally prefer TSH below 2.5 for fertility patients.
- Achieve or maintain a healthy body weight: Both underweight and overweight status can disrupt ovulation and hormonal balance. A BMI between 20 and 27 is generally associated with optimal fertility.
- Reduce chronic stress where possible: Chronic cortisol elevation suppresses reproductive hormones. This doesn’t mean “just relax” (a spectacularly unhelpful phrase in fertility conversations). It means building in genuine recovery: sleep, movement, social connection, and practices like yoga or mindfulness if they suit you.
3. Know Your Preservation Options
If you’re not ready to conceive now but want to keep your options open, egg freezing (oocyte cryopreservation) has become a medically sound, increasingly accessible option. The American College of Obstetricians and Gynecologists provides guidance on fertility preservation, noting that younger eggs (frozen in your early 30s rather than late 30s) yield better outcomes.
The process involves ovarian stimulation, egg retrieval under sedation, and cryopreservation. It does not guarantee a future pregnancy, but it gives you a hedge against further decline.
Success rates vary by age at freezing, clinic, and individual response to stimulation. Ask for clinic-specific data when evaluating providers, specifically live birth rates per egg retrieved, stratified by age.
4. Don’t Navigate This Alone
The fertility journey, at any stage, is emotionally complex. Whether you’re just beginning to notice signs or you’re deep in a treatment protocol, community matters.
Peer-reviewed support groups, therapists who specialize in reproductive health, and resources like RESOLVE: The National Infertility Association can make the difference between feeling isolated and feeling supported.
Your partner, if you have one, should also be involved early. Male factor infertility accounts for approximately 30 to 40% of fertility issues across couples. A semen analysis is a simple, non-invasive test that should happen early in any fertility evaluation, not as a last resort.
The Bottom Line: Your Fertility After 30 Is Not a Verdict, It’s a Conversation
Here’s the thing about fertility decline after 30. It is real, it is normal, and it is not a life sentence.
Women conceive in their 30s every day. Women with diminished ovarian reserve conceive. Women who have experienced miscarriage go on to have healthy pregnancies. Women who catch these signs early and take strategic action expand their options dramatically compared to those who wait.
What changes after 30 is not that pregnancy becomes impossible. What changes is that time becomes a more active participant in the equation. The signs in this article are your early warning system. The tests and steps outlined are your response protocol.
The Most Important Thing You Can Do Today
If you’ve read this far and you’re recognizing yourself in one or more of these signs, the most important thing you can do is not spiral into anxiety. It’s act.
Book an appointment with a reproductive endocrinologist for a fertility assessment, even if you’re not actively trying to conceive right now. The information you gain from a single consultation and a hormone panel can change how you plan the next two to five years of your life. It can tell you whether your timeline has more flexibility than you thought, or whether moving sooner makes more sense than you realized. Either answer is useful.
Many fertility clinics now offer “fertility check” packages specifically designed for women in their late 20s and 30s who want a snapshot of their reproductive health without committing to fertility treatment. These typically include an AMH test, Day 3 hormones, an antral follicle count ultrasound, and a consultation to interpret the results. They are, in most cases, well worth the investment in clarity alone.
A Note on the Emotional Weight of This Topic
Fertility is not just a medical topic. It is deeply personal, often tied to a woman’s sense of identity, her relationship, her plans, and sometimes her grief. Whether you have experienced pregnancy loss, a difficult diagnosis, years of unexplained infertility, or simply a growing awareness that time is doing something you weren’t ready for, those feelings are real and they matter.
Engaging with this information from a place of self-compassion rather than self-blame makes an enormous difference. You did not cause your fertility to decline. Biology is not a punishment. And the fact that you are reading this, asking these questions, and seeking information is already an act of care toward your future self.
You deserve to understand your own body. You deserve information that is accurate, specific, and given without condescension or alarm. And you deserve the agency that comes from knowing what’s happening, why it’s happening, and what, concretely, you can do about it.
Start with one step. Book the appointment. Order the test. Start tracking. One step creates the next one.
CTA
Found this article useful? Share it with a friend who’s in her 30s and thinking about her fertility, because most women never see this information until they’re already in a clinic wondering what they missed.
Have a question or a sign you’ve noticed that wasn’t covered here? Drop it in the comments below. This is a conversation, not a lecture, and your experience matters.
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider or reproductive endocrinologist for personalized guidance.