Vaginal Dryness: 9 Proven Non-Hormonal Solutions
Nobody warned you about this part. Not your doctor, not your mother, and certainly not the stack of pregnancy books on your nightstand. Yet here you are, dealing with a symptom that makes wearing underwear feel like sandpaper and sex feel like a punishment. You deserve better, and you are absolutely not alone.
Vaginal dryness is one of the most common and least talked-about complaints in women’s health, affecting women across every decade of life, from their twenties all the way through menopause and beyond. According to the Cleveland Clinic, more than 15% of women under 50 experience vaginal dryness before menopause, and that number climbs to over 50% after menopause. But the conversation around solutions has, for too long, started and ended with hormones.
Here is the thing: hormones are not your only option, and for many women, they are not an option at all. If you are breastfeeding, a breast cancer survivor, sensitive to hormone therapy, or simply prefer a natural approach, there are real, evidence-backed solutions waiting for you. This guide covers nine of the most effective ones, explains exactly how to use each, and tells you what to realistically expect from each approach.
Whether your dryness appeared out of nowhere after delivery, crept in during perimenopause, or has been a quiet passenger since your last medication change, one of these solutions, or a combination of them, is about to change your daily life for the better.
What Actually Causes Vaginal Dryness and Why It Matters for Treatment
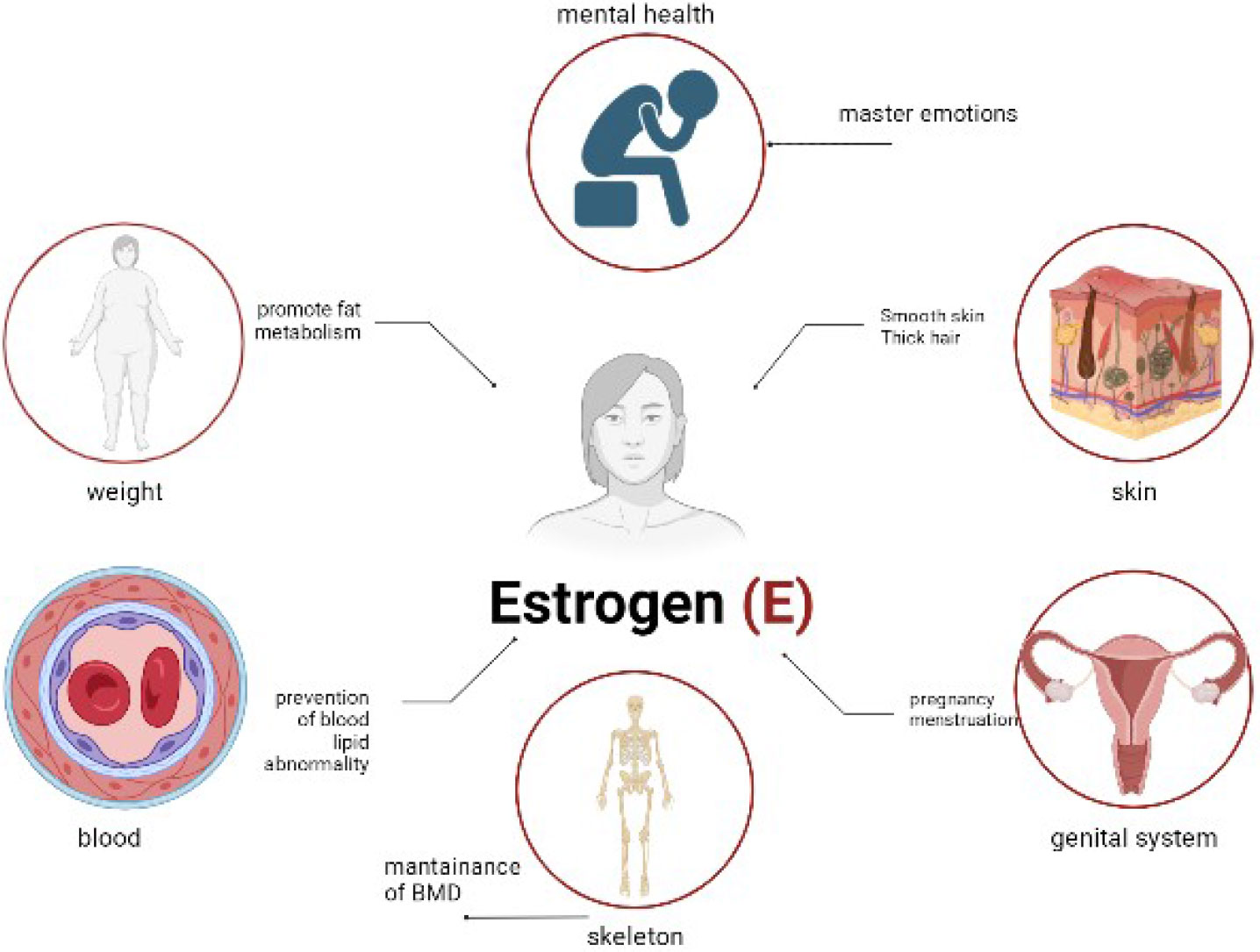
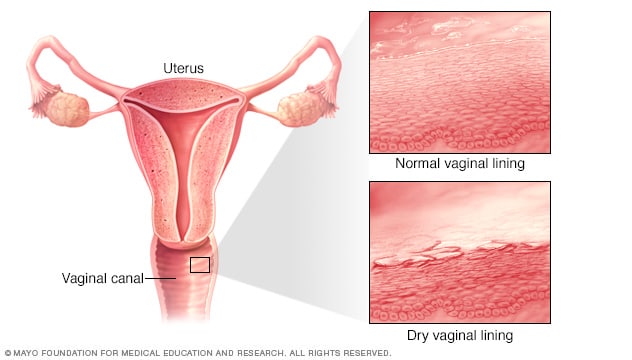
Before jumping into solutions, it helps to understand what is going on below the surface. Vaginal moisture depends heavily on estrogen. This hormone maintains the thickness, elasticity, and self-lubrication of vaginal tissue. When estrogen drops for any reason, the vaginal walls thin out and the tissue produces less natural fluid. The result is dryness, irritation, burning, and often pain during sex.
The tricky part is that estrogen can dip for many reasons, and this is why vaginal dryness is not just a menopause issue.
Common causes include:
- Breastfeeding. During lactation, the hormone prolactin rises to support milk production, and estrogen drops significantly. Research shows vaginal dryness is more than seven times more common in breastfeeding women than in those using infant formula.
- Perimenopause and menopause. As ovarian function declines, estrogen production slows, leading to progressive vaginal tissue changes.
- Certain medications. Antihistamines, some antidepressants, and hormonal birth control can all reduce natural lubrication as a side effect.
- Stress and anxiety. Mental stress increases cortisol, which in turn suppresses sex hormones and reduces blood flow to the genitals, directly reducing arousal and natural moisture.
- Cancer treatments. Chemotherapy, radiation to the pelvic area, and medications used in breast cancer treatment can all reduce estrogen levels significantly.
- Cigarette smoking. A 2017 study found that women who smoke are significantly more likely to experience vaginal dryness, as smoking accelerates the breakdown of estrogen and damages vaginal tissue cells.
- Harsh soaps and douching. Products with fragrances or aggressive chemicals disrupt the vagina’s natural pH, stripping away protective moisture.
Understanding your particular cause helps you choose the most targeted solution. A breastfeeding mother and a 54-year-old woman in menopause may both experience dryness, but their most effective first-line treatment might look slightly different.
Solution 1: Water-Based Vaginal Lubricants for Instant Vaginal Dryness Relief
Think of lubricants as the immediate first responders of vaginal dryness treatment. They do not fix the underlying tissue changes, but they do one job extraordinarily well: they eliminate friction, right now, when you need them most.
Water-based lubricants are the most widely recommended option. They are compatible with latex condoms, easy to clean up, and gentle on vaginal tissue. Look for formulas that are pH-balanced, fragrance-free, and free from glycerin (which can trigger yeast infections in some women). Popular well-tolerated options include Sliquid H2O, Good Clean Love, and Astroglide Natural.
How to use them correctly:
- Apply to both the vaginal opening and the partner’s body, or toy, immediately before sexual activity.
- Reapply as needed throughout. Dryness mid-session is not a personal failure; it is biology.
- Avoid products containing parabens, glycerin, or propylene glycol if you have a history of yeast infections or vulvar sensitivity.
What to expect: Instant improvement in comfort during intercourse. Lubricants do not provide long-term hydration or repair vaginal tissue, so they work best when paired with a regular moisturizing routine.
Symptoms helped: Pain during sex (dyspareunia), friction, tearing or micro-abrasions, and burning during intercourse.
Solution 2: Silicone-Based Lubricants for Long-Lasting Vaginal Dryness Comfort
Silicone lubricants are the marathon runners in the lubricant world. They last significantly longer than water-based formulas, do not dry out mid-session, and require less frequent reapplication. For women with more severe dryness, this makes a noticeable difference.
Silicone is also an excellent choice for water-based activities, since it is not water-soluble. It does not absorb into skin, which means it stays where you put it. Well-regarded options include Überlube, Pink, and ID Millennium.
How to use them correctly:
- Apply a small amount to the vaginal opening before sex. A little goes a long way with silicone.
- Do not use silicone lubricants with silicone sex toys, as the formula can degrade the toy material.
- Use with latex and polyurethane condoms safely. They are fully condom-compatible.
What to expect: Longer-lasting lubrication than water-based formulas, with a silkier feel. These are purely functional for sexual activity and, like water-based options, do not address underlying tissue health.
Symptoms helped: Severe friction and pain during sex, reduced sensation, and discomfort that persists throughout intercourse.
Solution 3: Vaginal Moisturizers for Ongoing Non-Hormonal Vaginal Dryness Treatment
Here is the distinction that most women are not told: lubricants are for sex, and moisturizers are for healing. A vaginal moisturizer is applied regularly, several times per week, whether you are having sex or not. It works by hydrating the vaginal tissue itself, restoring the mucosa’s natural moisture balance over time.
This is the category where the science gets genuinely exciting. Studies have found that regular use of vaginal moisturizers can produce results comparable to low-dose topical estrogen for women with mild to moderate symptoms. The Mayo Clinic recommends options like Replens, K-Y Liquibeads, and Sliquid as reliable first-line choices.
How to use them correctly:
- Apply internally using an applicator or your finger, typically at bedtime to minimize mess.
- Use every two to three days consistently for the best results, not just when you feel symptomatic.
- Give it time. Most women see meaningful improvement within four to eight weeks of regular use.
What to expect: Reduced daily irritation, improved tissue comfort even without sexual activity, and better baseline moisture that makes sex more comfortable when it happens.
Symptoms helped: Constant burning or itching, irritation from clothing, urinary discomfort, and pain during gynecological exams.
Solution 4: Hyaluronic Acid Suppositories, the Standout Star of Non-Hormonal Vaginal Dryness Relief
If you follow skincare science at all, hyaluronic acid is a name you know. It is one of the body’s natural humectants, meaning it binds to water and locks in moisture. What is less widely known is that the same mechanism that makes it a skincare powerhouse also makes it one of the most promising non-hormonal vaginal dryness treatments available.
When applied internally, hyaluronic acid adheres to the vaginal epithelial cells and draws water into the tissue, hydrating from the inside out. A landmark multicenter randomized controlled trial found that hyaluronic acid vaginal gel was comparable in effectiveness to estriol vaginal cream for reducing dryness and improving vaginal health scores. That is a significant finding, especially for women who cannot use any form of estrogen.
According to Mayo Clinic Press, vaginal moisturizers containing hyaluronic acid are among the most effective non-hormonal treatments available, with most women noticing meaningful improvement after eight to twelve weeks of regular use.
How to use them correctly:
- Insert a suppository or gel applicator into the vagina at bedtime, at least every three days.
- Look for pH-balanced, fragrance-free, paraben-free formulations specifically designed for vaginal use.
- Popular options include Revaree by Bonafide, Hyalogyn, and Good Clean Love’s suppositories.
What to expect: Progressive improvement in daily comfort, tissue elasticity, and lubrication during sex. Unlike lubricants, the effect builds over time and continues even on days when you do not apply it.
Symptoms helped: Persistent dryness and burning, painful intercourse, reduced elasticity, irritation independent of sexual activity.
Solution 5: Pelvic Floor Physical Therapy for Vaginal Dryness and Intimacy
This one often surprises people. Physical therapy, for vaginal dryness? Yes, genuinely. And it is arguably the most underutilized, most transformative option on this entire list.
The pelvic floor is a group of muscles that support the uterus, bladder, and rectum. When these muscles are tight, overactive, or poorly coordinated, they restrict blood flow to the vaginal tissues, exacerbate pain during sex, and can amplify the experience of dryness even when moisture levels are not dramatically low. A pelvic floor physical therapist can assess exactly what your muscles are doing and guide you through targeted work to restore normal function.
For women who have experienced dyspareunia (painful sex) for an extended time, a common secondary pattern develops: the body begins to tense the pelvic floor in anticipation of pain. This protective bracing actually makes discomfort worse. A skilled therapist can interrupt this cycle through manual therapy, guided relaxation techniques, and a progressive home program.
What a typical program looks like:
- An initial assessment of pelvic floor muscle tone, coordination, and strength.
- Internal and external manual therapy to release tight or tender tissue.
- Instruction in diaphragmatic breathing, which directly reduces pelvic floor tension.
- A home exercise program that may include both relaxation and strengthening, depending on your specific pattern.
What to expect: Noticeable reduction in pain during sex, improved tissue comfort, and better overall pelvic awareness, typically within six to twelve weeks of regular therapy.
Symptoms helped: Painful intercourse, pelvic heaviness, urinary urgency or leakage, muscle tension that compounds dryness-related discomfort.
Solution 6: Kegel Exercises to Improve Blood Flow and Vaginal Lubrication Naturally
Kegel exercises are the most well-known pelvic floor exercise, and for good reason. Named after gynecologist Dr. Arnold Kegel, these rhythmic contractions of the pelvic floor muscles strengthen the muscles that surround the vagina and increase circulation to the entire region. Better blood flow means better tissue health, better arousal response, and, over time, improved natural lubrication.
The key word in that sentence is “natural lubrication.” While Kegels are not a replacement for topical treatments, they support your body’s own capacity to produce moisture, especially when performed consistently alongside other solutions.
How to perform them correctly:
- Identify the right muscles by imagining you are stopping the flow of urine mid-stream. Those are your pelvic floor muscles.
- Squeeze and lift these muscles for three to five seconds, then fully release for an equal amount of time.
- Aim for three sets of ten repetitions daily. Fully releasing after each squeeze is just as important as the contraction itself.
- Do not hold your breath or squeeze your buttocks, thighs, or abdomen. The work should be isolated.
A common mistake: Many women with pelvic pain have a pelvic floor that is already too tight. If Kegels worsen your discomfort rather than helping, stop and consult a pelvic floor physical therapist before continuing.
What to expect: Gradual improvement in pelvic circulation, better bladder control, and enhanced arousal response over six to twelve weeks of consistent practice.
Symptoms helped: Urinary leakage, reduced vaginal sensation, pain during intercourse related to poor muscle tone, and reduced arousal.
Solution 7: Diet, Hydration, and Phytoestrogens for Vaginal Dryness Support
What you eat and drink has a more direct effect on vaginal moisture than most women realize. The tissue of the vaginal wall requires adequate hydration to maintain its suppleness. Chronic mild dehydration is a quiet contributor to dryness that many women overlook entirely.
Drinking at least eight cups of water daily is a simple, no-cost starting point. Beyond hydration, certain foods offer compounds that gently support estrogen-related tissue health without functioning as hormones in the clinical sense.
Phytoestrogens are plant compounds that weakly mimic the action of estrogen in the body. They are found naturally in many foods and have been studied for their potential to ease vaginal dryness, particularly in postmenopausal women. Research published by MedlinePlus suggests that a diet rich in soy foods may improve vaginal dryness symptoms due to the phytoestrogen isoflavone content.
Foods that support vaginal tissue health:
- Soy products (tofu, tempeh, edamame): Rich in isoflavones, the most studied phytoestrogens.
- Flaxseeds and walnuts: High in omega-3 fatty acids, which support tissue membrane integrity and moisture retention.
- Avocado: Contains healthy fats linked to hormone production and improved vaginal lubrication.
- Leafy greens (spinach, kale): High in magnesium, which plays a supportive role in hormone balance.
- Pumpkin seeds and almonds: Zinc-rich foods associated with hormonal balance and improved libido.
What to expect: Dietary changes are slow-acting but cumulative. Combined with topical solutions, a supportive diet can meaningfully reduce dryness symptoms over two to three months.
Symptoms helped: Chronic dryness linked to dietary deficiency, reduced tissue elasticity, general inflammation in vaginal tissues.
Solution 8: Eliminating Irritants and Resetting Your Vaginal Environment for Dryness Relief
This solution is free, takes about ten minutes, and produces results faster than almost anything else on this list. Many cases of vaginal dryness and irritation are not caused by estrogen alone; they are worsened, sometimes dramatically, by everyday products that disrupt the vaginal environment.
The vagina is self-cleaning. It maintains its own carefully balanced pH, between 3.8 and 4.5, which is naturally slightly acidic. Disrupting this balance strips away the protective mucus layer and leaves tissue exposed, dry, and inflamed.
Common culprits to remove immediately:
- Scented soaps, body washes, and bubble baths used near the vulva or inside the vagina.
- Douches of any kind. There is no medical justification for douching, and strong evidence that it causes more harm than it prevents.
- Scented or dyed toilet paper and sanitary products. Unscented, fragrance-free products are always the better choice for sensitive tissue.
- Fabric softeners or laundry detergents with strong fragrances that remain in underwear fabric.
- Certain condom types with spermicide or flavoring that can cause significant local irritation.
Switching to gentle, unscented products and washing only the external vulva with warm water (or a mild, unfragranced soap) is the foundation of vaginal health maintenance. Think of it as removing the noise so you can hear what your body actually needs.
What to expect: For many women, eliminating irritants alone brings noticeable reduction in burning and itching within one to two weeks.
Symptoms helped: Burning, itching, discharge irregularity, contact irritation from clothing, and chemical-triggered dryness.
Solution 9: Extended Foreplay and Intentional Arousal Practices to Restore Comfort and Intimacy
This solution is the one most often omitted from clinical lists, which is a shame because it is both free and remarkably effective. Natural vaginal lubrication is primarily an arousal response. The Bartholin’s glands, located on either side of the vaginal opening, produce fluid when a woman is fully aroused. When sex is rushed, when arousal is incomplete, or when stress is high, these glands simply do not get the signal to activate fully.
This is not a performance issue. It is physiology. And the most straightforward way to address it is to give your body more time and more input before penetration.
Extended, intentional foreplay, defined as a minimum of fifteen to twenty minutes of arousal before penetrative sex, increases blood flow to the vaginal walls, stimulates the Bartholin’s glands, and promotes the trans-udate fluid that creates natural lubrication. For women already experiencing some level of dryness, this may not be sufficient on its own, but it reliably improves comfort when combined with a topical solution.
Practical approaches:
- Communicate with your partner about taking more time before intercourse. This conversation, though it might feel awkward once, almost always improves intimacy.
- Explore non-penetrative intimacy (massage, oral sex, mutual touch) during periods when penetrative sex is especially uncomfortable. These activities maintain connection without pressure.
- Mindfulness practices before sex, even five minutes of slow breathing or body-scan meditation, can reduce the pelvic muscle guarding that amplifies dryness-related pain.
- Reduce mental load before intimacy. Stress is one of the most potent suppressors of arousal, and arousal is the engine of natural lubrication.
What to expect: Improved natural lubrication during sexual activity, reduced pain, and greater emotional and physical satisfaction, particularly when combined with a regular moisturizer routine.
Symptoms helped: Low natural lubrication during sex, pain at penetration, reduced sensation, and intimacy avoidance driven by fear of discomfort.
Comparison Table: Non-Hormonal Vaginal Dryness Solutions at a Glance
| Solution | Type | Frequency of Use | Time to Results | Best For | Difficulty |
|---|---|---|---|---|---|
| Water-based lubricant | Topical | As needed (during sex) | Immediate | Instant comfort during sex | Very Easy |
| Silicone-based lubricant | Topical | As needed (during sex) | Immediate | Long-lasting friction relief | Very Easy |
| Vaginal moisturizer (polycarbophil) | Topical | 2 to 3x per week | 4 to 8 weeks | Daily dryness and irritation | Easy |
| Hyaluronic acid suppository | Topical | Every 2 to 3 days | 8 to 12 weeks | Tissue repair and deep hydration | Easy |
| Pelvic floor physical therapy | Clinical | Weekly sessions | 6 to 12 weeks | Pain during sex, muscle tension | Moderate |
| Kegel exercises | Self-directed | Daily | 6 to 12 weeks | Blood flow, bladder leakage, sensation | Easy to Moderate |
| Dietary changes and hydration | Lifestyle | Daily | 2 to 3 months | Systemic hormonal support | Easy |
| Eliminating irritants | Lifestyle | Ongoing | 1 to 2 weeks | Chemically triggered dryness | Very Easy |
| Extended foreplay and arousal | Behavioral | Per encounter | Immediate to gradual | Natural lubrication during sex | Moderate |
How to Build Your Personal Non-Hormonal Vaginal Dryness Protocol
The most effective approach is not choosing one solution from this list and hoping for the best. It is layering several complementary strategies to address the problem from multiple angles at once. Think of it as building a system rather than relying on a single fix.
A simple starting protocol might look like this. First, remove all potential irritants from your personal care routine immediately. Second, begin using a vaginal moisturizer or hyaluronic acid suppository every two to three days as your baseline treatment. Third, add a quality water-based lubricant for sexual activity. Fourth, commit to daily pelvic floor exercises or, better yet, consult a pelvic floor physical therapist if pain is part of your picture.
Support all of the above with adequate daily hydration and a diet that includes omega-3 fatty acids, leafy greens, and, if appropriate, soy-based phytoestrogens. Finally, give your intimate life the time it deserves by prioritizing full arousal before penetration.
Most women who follow a consistent multi-pronged approach like this see meaningful, lasting improvement within six to twelve weeks. That is not a long time given how significantly vaginal dryness affects daily comfort, confidence, and intimacy.
As the American College of Obstetricians and Gynecologists notes, vaginal dryness is a common and treatable condition, and women do not have to simply endure it. The solutions exist. Using them is an act of self-respect.
When to See a Doctor About Vaginal Dryness
Non-hormonal solutions work well for most women, but there are situations where a medical consultation is the right first step. See your gynecologist or healthcare provider if:
- Dryness is accompanied by unusual vaginal discharge, odor, or bleeding.
- You have tried over-the-counter solutions consistently for eight to twelve weeks without improvement.
- Pain during sex is severe enough to prevent intercourse or is getting progressively worse.
- You have a history of hormone-sensitive cancer and want guidance on the safest topical options.
- You experience symptoms of a urinary tract infection alongside dryness, including burning with urination, urgency, or frequency.
A pelvic exam, and sometimes a blood test to check hormone levels, can help identify whether an underlying condition is driving your symptoms and open the door to additional treatments, including prescription non-hormonal options, if needed.
The Bottom Line: Vaginal Dryness Is Common, Treatable, and Not Your Fault
Vaginal dryness is not a sign of age, failure, or anything wrong with you as a person. It is a physiological response to changes in hormone levels, lifestyle factors, and occasionally the products in your bathroom cabinet. And it responds well to treatment.
You do not need to choose between suffering in silence or immediately reaching for a prescription. Nine legitimate, evidence-backed non-hormonal solutions are on this list, and at least three of them can be started today, for free, with things you already own or can buy at any pharmacy.
Start where you are. Make one change, and then another. Your body is not working against you. It just needs a little support.
Keep the Conversation Going
Did this help? Share this post with a friend, a sister, or a new mom who has been quietly dealing with the same thing and does not know where to start. The more openly we talk about this, the sooner women stop suffering for years before finding the solutions that were available all along.
Read Next: [Pelvic Floor Health After Baby: What No One Tells You in the First Year]
Drop a comment below: Which of these solutions have you tried? What worked for you? Your experience might be exactly what someone else needs to read today.
This article is for informational purposes only and does not constitute medical advice. Please consult your healthcare provider before beginning any new treatment, especially if you have a history of hormone-sensitive conditions.